Dual-energy CT achieves high sensitivity and excellent negative predictive value in more overt cases of traumatic bone marrow lesions in ankle joints, but it performs poorly with more subtle changes as seen on MRI, researchers reported online May 8 in Radiology.
While the Swiss group believes dual-energy CT's diagnostic performance is related to the degree of bone marrow abnormality on MRI, information garnered from dual-energy CT still may help clinicians rule out distinct bone marrow lesions in patients with dramatic ankle injuries.
The lead author of the study is Dr. Roman Guggenberger from the department of radiology at University Hospital Zurich.
Ankle fractures
Past studies have shown that the ankle is the most commonly injured joint in the body, with fractures as the most common abnormality. While MRI has traditionally been the modality of choice to detect bone marrow lesions, it is not always routinely performed on patients with ankle trauma or in cases when x-ray and CT images are negative for fractures.
Dual-energy CT has improved the ability of the modality to characterize and differentiate body substances with high anatomic composition of iron, calcium, or iodine, the authors noted. Based in part on previous research, Guggenberger and colleagues speculated that dual-energy CT with reconstruction of noncalcium images could detect traumatic bone marrow lesions in the ankle joint.
 |
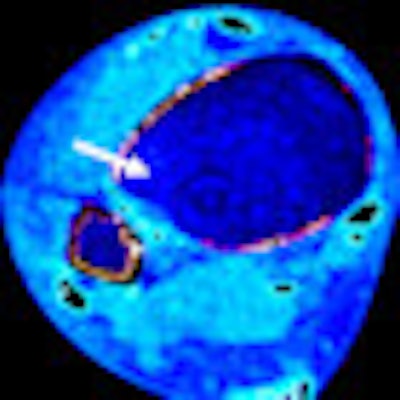
| Transaxial images at the tibial pilon of the right ankle joint in a 40-year-old woman with acute ankle trauma. T2-weighted short-tau inversion recovery (STIR) MR image (left) shows subtle bone marrow lesion in the lateral aspect of the anterior tibial pilon (arrow). Weighted-average image simulating single-energy CT (right) shows no fracture (arrow). |
 |
| Gray level-coded (left) and color-coded noncalcium dual-energy CT (right) confirm no bone marrow abnormalities (arrow) and a false-negative result. All images courtesy of Radiology. |
Between September 2010 and May 2011, 30 consecutive patients (15 women and 15 men; mean age, 34.7 years) who were suspected to have fractures as seen on x-ray were referred for CT with acute ankle trauma.
Researchers excluded patients younger than 18 years of age, women who were pregnant, and patients with contraindications for MRI, such as non-MRI-compatible pacemakers. They also omitted individuals with prior ankle trauma, those who had surgery within one year of the current trauma, and those with metal implants.
Scanning protocol
All CT scans were obtained with a second-generation 128-slice dual-source CT scanner (Somatom Definition Flash, Siemens Healthcare). MRI exams were performed on a 1.5-tesla system (Signa Excite HDx, GE Healthcare) with a dedicated eight-channel ankle coil.
The researchers subdivided the ankle joints into 10 anatomic regions, which then were evaluated for traumatic bone marrow lesions on the noncalcium dual-energy CT images. Two independent readers unaware of the MRI results used a four-point classification system, in which grade 1 indicated distinct signs of abnormal bone marrow attenuation and grade 4 represented normal bone marrow.
Guggenberger and colleagues only included traumatic bone marrow lesions that were more than 3 mm from the adjacent cortical bone. This was because artifacts from beam hardening, removal of cortex, and filtering effects on noncalcium dual-energy CT images were expected to potentially interfere with the analysis of the bone marrow in this area.
All MR images were evaluated for the presence of traumatic bone marrow lesions by a third reader in random order. The reader was blinded to the CT results and used the same four-point classification system.
Reader results
In reviewing the images, fractures were found on CT images in six (20%) of 30 patients. MRI showed traumatic bone marrow lesions in 60 (20%) of 300 regions. In eight (13%) of those 60 regions, lesions were smaller and within 3 mm of the cortical bone and therefore excluded from further analysis. The remaining 52 anatomic regions with traumatic bone marrow lesions were included in the study.
By including grade 1 and grade 2 lesions as positive for bone marrow lesions based on MRI, there were 16 false-negative and 38 false-positive findings with dual-energy CT. Overall interreader agreement for grading the dual-energy CT images was substantial (κ = 0.66).
Of the 16 false-negative findings on dual-energy CT, 14 (87%) regions received grade 2 classification and two (12%) received grade 1 on MRI. Of the 38 false-positive CT findings, 30 (79%) regions received grade 3 classification, with eight (21%) regions evaluated as grade 4 on MRI.
When including in the analysis only grade 1 lesions as positive for bone marrow lesions according to MRI results, the sensitivity of dual-energy CT increased to 90% for both readers, while specificity decreased to 82% and 81%. Positive predictive value also declined to 27% and 25% for the two readers. Negative predictive value increased to 99% for both readers, while accuracy remained steady at 82% and 81%.
Image interpretation
Based on the results, Guggenberger and colleagues concluded that dual-energy CT can diagnose traumatic bone marrow lesions in patients with acute ankle trauma with high sensitivity and excellent negative predictive value, when strict image interpretation criteria for the presence of traumatic bone marrow lesions on MRI are used.
However, when subtle bone marrow lesions from MR images were included in the evaluations, dual-energy CT was less sensitive, and its negative predictive value was lower. "Irrespective of the interpretation criteria used for MR imaging, the specificity, and in particular the [positive predictive value], of dual-energy CT for the diagnosis of traumatic bone marrow abnormalities remains poor," they wrote.
The authors cited several limitations to the study, including the small sample size of only 30 patients with acute ankle trauma. They also noted the exclusion of lesions within 3 mm of the cortical bone due to potential artifacts, as well as the relatively young study population; results may have differed in an elderly population with osteopenia.
| One study co-author, Bernhard Krauss, PhD, is employed in the department of CT at Siemens Healthcare's Imaging and Therapy Division. The study noted that all authors who are not employees of or consultants for Siemens had control of inclusion of any data and information that might present a conflict of interest for Krauss. |



















