A Turkish study on the diagnosis and management of breast cancer with bone metastasis found that while the country largely complies with international guidelines, physicians need to increase their awareness and knowledge of the current guidelines.
The researchers from various institutions across Turkey also pointed out the need to provide breast imaging clinics with the necessary equipment to achieve optimal and standardized management of bone metastasis.
Breast cancer, one of the most common malignancies amongst Turkish women, frequently metastasizes to the bone: Approximately 70% of patients with recurrent breast cancer have bone metastasis, a common cause of morbidity and mortality, noted lead author Dr. Ali Arican, from the department of medical oncology at Mersin University Hospital, and colleagues.
Managing the condition is complex and challenging, and effective management requires practical guidelines, they wrote.
 Dr. Ali Arican from Mersin University Hospital.
Dr. Ali Arican from Mersin University Hospital.There are few international guidelines for metastatic breast cancer, particularly for managing bone metastasis in these patients. One set is the British Association of Surgical Oncology (BASO) guidelines.
The BASO guidelines were developed by a multidisciplinary group of specialists and consider all aspects of care of metastatic bone disease, including diagnosis, staging, treatment, and assessing the response to treatment.
"Our aim was to address the current clinical practice of breast cancer patients with bone metastasis in Turkey," Arican said in an interview with AuntMinnie.com. "We decided to compare our practice in managing bone metastasis in breast cancer patients with international guidelines from BASO."
In their paper, which was published online April 22 in Supportive Care in Cancer, the authors noted that there is no current research on management practices for breast cancer patients with bone metastasis in Turkey, and there are no widely accepted national guidelines. Identifying current clinical approaches and their rate of compliance to international guidelines would provide a basis for developing national guidelines and policies for managing these patients.
Arican and colleagues conducted a multicenter, cross-sectional, epidemiological survey in 38 centers across Turkey between December 2010 and June 2011 to determine the compatibility of Turkish management practices with the BASO guidelines.
They included 1,026 patients with a mean age of 54. Of these patients, 801 (78.1%) were premenopausal and 225 (21.9%) were postmenopausal. All patients had histologically diagnosed breast cancer, radiologically proven bone metastasis, and a life expectancy of more than six months.
The authors recorded information about physical examination methods, radiological tools, interventional techniques, pathology and laboratory methods used for diagnosis, surgical approaches, chemotherapy, radiotherapy, bisphosphonate use, supportive treatment, and other treatment regimens used at the centers.
They then determined adherence to the BASO guidelines for four aspects of care for metastatic bone disease: diagnosis, staging, treatment, and assessment of treatment response.
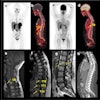
The imaging modality used most often for diagnosing bone metastasis was bone scintigraphy (57.8%), followed by radiography (22.8%), the group found. Bone biopsy and fine-needle aspiration biopsy were used as the diagnostic methods in only 46 patients (4.5%).
Tumor markers were detected in 94.9% of the study population, and markers of bone metabolism were measured in 90.4% of patients. Of the 1,026 patients, 3.5% underwent surgery, 26.4% received palliative chemotherapy, 56.5% received radiotherapy, and 10.4% had hormonal therapy for bone metastasis.
Consistent with the guidelines, most of the patients (96%) received bisphosphonates, most commonly ibandronic acid and zoledronic acid. For the postoperative follow-up of bone metastasis, radiography, bone scintigraphy, and CT were three main imaging tools, consistent with the BASO guidelines.
The authors declared their findings to be more than 95% consistent with the BASO guidelines for the use of radiological methods and laboratory tests to diagnose and stage bone metastasis, and for the use of chemotherapy and hormonal therapy for bone metastasis.
However, interventional procedures such as biopsy for diagnosing bone metastasis and surgical treatment were applied to a much lesser extent than recommended by the BASO guidelines, they noted. The low rate of surgery could be due to the lack of involvement in patient care by orthopedic surgeons and neurosurgeons.
Finally, while the use rate of radiotherapy was higher, it was still less than suggested in the BASO guidelines.
The authors stressed the importance of a multidisciplinary approach including radiation oncologists, medical oncologists, orthopedic surgeons, neurosurgeons, and radiologists to achieve the optimum therapeutic approach for bone metastasis.
Few studies have included such a large number of breast cancer patients with bone metastasis, and these results have implications regarding medical practice in Turkey, according to Arican.
Overall, there was good adherence to international guidelines; the only major difference was the low bone biopsy rate for interventional purposes by orthopedists and neurosurgeons, he added.
Arican also pointed out that awareness and equipment for appropriate interventional procedures should be supported in every clinic to obtain the adequate adherence to current guidelines.
"Radiology -- especially MRI -- has high importance in diagnosis and follow-up for these patients in evaluating the skeletal system," he concluded. "Access to these modalities is not a common issue in the 38 centers that we [examined] in this study, so we have found that the equipment, access, and utilization of these modalities are adequate in our practice."