Varicella-Zoster Pneumonia
Clinical:
Varicella-Zoster pneumonia can occur in 5 to 50% of cases of varicella infection in adults (more than 90% of cases of varicella-zoster pneumonia occur in adults). Immunosuppressive conditions such as lymphoreticular malignancy, steroids, pregnancy, COPD, and severe cutaneous manifestations increase the risk for developing pulmonary infection.Patients can exhibit a wide range of clinical findings from asymptomatic to severe pulmonary infection with respiratory arrest and death (up to 11-20% of cases). The pneumonia usually develops within a few days of the skin rash. When pneumonia develops the skin rash is usually severe and often extends to the mucosa of the mouth and pharynx.
X-ray:
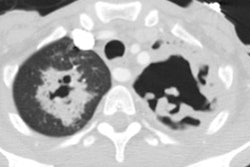
On plain film, varicella pneumonia produces multiple 5 to 10 mm ill-defined nodules that may become confluent. Adenopathy and effusions are unusual [2].Findings on HRCT include numerous 1-10 mm well-defined and ill-defined nodules throughout both lungs. Other findings include nodules with surrounding ground-glass attenuation ("halo sign"), patchy ground-glass attenuation and consolidation, and coalescence of nodules [1]. In a small number of patients the lesions will calcify with healing resulting in numerous randomly distributed 2 to 3 mm dense nodules [4].
REFERENCES:
(1) AJR 1999; Kim JS, et al. High-resolution CT findings of varicella-zoster pneumonia. 172: 113-116
(2) Radiographics 2002; Kim EA, et al. Viral pneumonias in
adults:
radiologic
and pathologic findings. 22: S137-S149
(3) Radiology 2011; Franquet T. Imaging of pulmonary viral
pneumonia. 260: 18-39
(4) Radiographics 2018; Koo HJ, et al. Radiographic and CT features pf viral pneumonia. 38: 719-739