Bacillary Angiomatosis:
Clinical:
Bacillary angiomatosis is a rare infection secondary to the organism Bartonella (Rochalimaea) henselae (the cat-scratch fever agent - a gram negative bacillus that stains with Warthin-Starry stain) seen almost exclusively in HIV patients (generall with advanced immunosuppression- CD4 counts below 100-200 cells/uL). Exposure to cats, cat fleas, and lice are the main risk factors for infection [3]. The infection results in very vascular lesions with marked capillary proliferation noted most commonly in the skin, followed by the bones, liver, spleen, lymph nodes, and lungs [4. Characteristic purplish skin lesions may be confused with those of Kaposi's sarcoma- the lesions are well circumscribed, tender, friable erythematous and bleed easily. Polypoid, exophytic endotracheal and endobronchial lesions have also been reported and may mimic the appearance of Kaposi's sarcoma bronchoscopically. Multiorgan involvement is common and skeletal disease (lytic bone lesions) can aid in the differentiation of this infection from Kaposi's sarcoma. Peliosis hepatis (dilated blood filled spaces) can also occur. Disseminated infection is characterized by fever, night sweats, weight loss, anemia, occasional hemoptysis [3], and elevated sedimentation rate. Treatment is with erythomycin, doxycycline, clarithromycin, or antibiotics directed against mycobacterial disease. Response to antibiotic therapy is rapid with improvement in only a few days and total resolution within about 3 weeks. Unfortunately, relapses can occur following cessation of antibiotic therapy. Without treatment the infection is progressive and can be fatal.
X-ray:
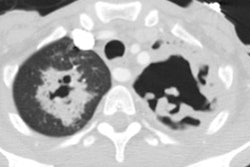
The radiographic findings most commonly consist of small nodules (1.5 mm to 1.5 cm) and the margins can be well or ill-defined. Associated markedly enhancing mediastinal adenopathy and pleural effusions are common. The lung nodules themselves may also densely enhance after contrast administration. There are caserports of endobronchial polyps occurring in the disease [4]. Abdominal periaortic adenopathy, low attenuation liver and spleen lesions, and ascites may also be seen. Bone lesions are lytic or permeative and painful.
REFERENCES:
(1) Radiology 1995; 197: 67-72
(2) Radiologic Clinics of North America 1997; McGuinness G. Changing trends in the pulmonary manifestations of AIDS. 35 (5): 1029-1082 (Review)
(3) AJR 2003; Brecher CW, et al. CT and radiography of bacterial
respiratory
infections in AIDS patients. 180: 1203-1209
(4) AJR 2012; Lichtenberger JP, et al. What a differetial a virus makes: a practical approach to thoracic imaging findings in the context of HIV infection- Part I, pulmonary findings. 198: 1295-1304