J Nucl Med 1998 Dec;39(12):2080-4
Lymphoscintigraphy and radioguided biopsy of the sentinel axillary node in
breast cancer.
De Cicco C, Cremonesi M, Luini A, Bartolomei M, Grana C, Prisco G, Galimberti V,
Calza P, Viale G, Veronesi U, Paganelli G.
Lymphoscintigraphy associated with radioguided biopsy of the sentinel node (SN)
is well established in clinical practice for melanoma. In breast cancer, the SN
concept is similarly valid, and lymphoscintigraphy is a useful method for
localizing the axillary SN. The aim of this study was to optimize the
lymphoscintigraphy technique in association with a gamma ray detecting probe
(GDP) for identifying and removing the SN in breast cancer patients. METHODS:
Two-hundred fifty patients with operable breast tumor underwent
lymphoscintigraphy before surgery. Three different size ranges of 99mTc-labeled
colloid particles (<50, <80 and 200-1000 nm) were used, with either
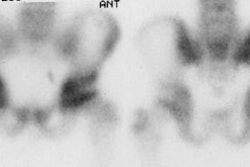
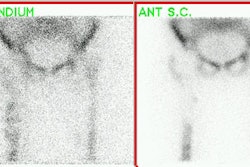
subdermal (above tumor) or peritumoral injection. Early and late scintigraphic
images were obtained in anterior and oblique projections, and the skin
projection of the detected SN was marked. Sentinel nodes were identified and
removed with the aid of the GDP during breast surgery; they were tagged
separately. Complete axillary dissection followed. In 40 patients, a blue dye
was also administered in addition to subdermal radiolabeled colloid to compare
blue dye mapping with lymphoscintigraphy localization. RESULTS:
Lymphoscintigraphy successfully revealed lymphatic drainage in 245 of 250
patients (98%). The axillary SN was identified in 240 patients (96%). SN biopsy
correctly predicted axillary node status in 234 of 240 patients (97.5%).
Lymphoscintigraphy and GDP detected the SN most easily and consistently when
200-1000 nm colloid was administered subdermally in an injection volume of 0.4
ml. Blue dye mapping was successful in 30 of 40 patients (75%). In 26 of these
patients, the dye and lymphoscintigraphy identified the same node; in 4 cases
different nodes were identified. None of these four patients had axillary
disease. CONCLUSION: Lymphoscintigraphy is a simple procedure that is well
tolerated by patients. Sentinel node identification is more reliable when
large-size radiolabeled colloids are injected in a relatively small injection
volume (0.4 ml). Use of a GDP greatly facilitates precise pinpointing and rapid
removal of the SN.