CHICAGO - Computer-aided detection (CAD) technology can yield high sensitivity in detecting amorphous calcifications on full-field digital mammography (FFDM) images, according to research presented Tuesday at the 2010 RSNA meeting in Chicago.
In a retrospective study targeted at amorphous calcifications, researchers from Princess Margaret Hospital in Toronto found that CAD correctly marked all breast cancers, 85% of high-risk lesions, and 80% of benign amorphous calcifications.
Amorphous calcifications are frequently overlooked by radiologists, and previous studies have showed low sensitivity for these lesions from the use of CAD software with digitized film-screen mammograms (i.e., indirect CAD), according to presenter Anabel Scaranelo, MD, PhD.
The researchers sought to evaluate if a CAD system applied to FFDM images could improve on this performance. From a database search of 1,438 consecutive stereotactic-guided biopsies between February 2001 and November 2006, the study team selected FFDMs from 122 women with a total of 124 biopsy-proven amorphous calcifications.
The women had a mean age of 56, with an age range of 35 to 84. All cases received a standard FFMD exam on a system from GE Healthcare of Chalfont St. Giles, U.K. Version 7.2 of the Second Look CAD software (iCAD, Nashua, NH) was applied.
For the purposes of the study, amorphous calcifications meant "microcalcifications sufficiently small or hazy that a more specific morphologic classification cannot be made," Scaranelo said. Of the 124 lesions, 36 (30%) were cancers, including five invasive and in situ and 31 in situ. There were 13 high-risk lesions and 75 benign lesions.
The cases all received mammographic follow-up for at least two years. The researchers noted mammographic density, size, and distribution of the lesions, and also evaluated patient risk factors.
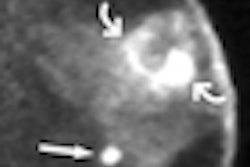
CAD findings were considered to be true-positive if a CAD marked at least one area of the mammographic location of the cancer or high-risk lesion. False-negative findings occurred when the biopsy-proven cancer or high-risk lesion was not marked by the CAD software.
False-positive findings were recorded if at least one view of the mammographic location of a benign amorphous calcification was marked or if ellipses and rectangles highlighted potential areas of concern not related to the area biopsied.
The CAD software correctly marked all 36 cancers for 100% sensitivity. "That's much higher when we compare with the literature using indirect CAD," she said.
CAD also detected 11 of 13 high-risk lesions for 85% sensitivity. Combining both cancers and high-risk lesions into one group, CAD turned in 96% sensitivity, 80% specificity, and 86% accuracy. The likelihood of malignancy in this group was 29%.
Looking at the data further by breast density, CAD had 100% sensitivity and 75% specificity for breast lesions with ACR BI-RADS breast density category 1 and 2. In dense breasts (ACR category 3 and 4), CAD had sensitivity of 93% and specificity of 85%. No significant difference was found between marking of fatty and dense breasts (p > 0.05).
Small differences were found for lesion size, however. In 1-7 mm lesions, CAD offered 96% sensitivity, 75% specificity, and 82% accuracy. For lesions ≥ 7 mm in extension, CAD led to 95% sensitivity, 95% specificity, and 95% accuracy.
In other findings, the false-positive rate was 1.76 marks per four-image case.
By Erik L. Ridley
AuntMinnie.com staff writer
November 30, 2010
Related Reading
FFDM plus MRI boosts mammography CAD performance, September 28, 2010
Double readers top CAD in finding breast tissue deformities, July 26, 2010
U.K. study finds mammo CAD can save money, November 9, 2009
Why are correct CAD marks ignored? It's anybody's guess, November 9, 2009
CAD finds breast cancers missed at CR mammography, July 31, 2009
Copyright © 2010 AuntMinnie.com