CHICAGO - Low-dose coronary CT angiography (CTA) delivered far less DNA damage than conventional coronary angiography, researchers from Berlin reported on Monday at the RSNA meeting's cardiac imaging sessions.
Using prospective electrocardiogram triggering at 320-detector-row CT produced only a fraction of the damage seen at conventional angiography, based on a validated technique for measuring genetic damage from double-strand breaks in DNA.
Exposure to ionizing radiation "can lead to DNA double-strand breaks, which according to the site of the damage can lead to chromosomal aberrations ... and carcinogenesis, even if the damage occurs only in a single cell," explained Dominik Geisel, MD, from Charité University Hospital in Berlin.
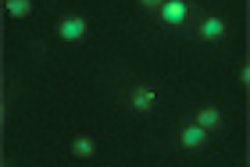
The extent of this DNA damage can be assessed accurately using a novel technique known as immunofluorescence microscopy, he said. Damage to the patient's blood lymphocyte DNA is used in the technique as a surrogate for more generalized genetic damage following exposure to ionizing radiation from imaging exams.
The technique works as follows: Within the DNA of patients' blood lymphocytes, the histone variant H2X is phosphorylated when exposed to radiation, and the resulting γH2AX antibodies can be visualized using fluorescence microscopy. After staining, researchers simply count the bright green foci within the cell nuclei under the microscope, each of which represents a double-strand break, Geisel said. Previous studies have compared DNA damage in retrospectively-gated versus prospectively-gated CTA, and conventional coronary angiography versus CT coronary angiography.
The study aimed to prospectively compare the biological effects of radiation exposure, measured as DNA double-strand breaks (DSBs), of 320-detector-row cardiac CT with diagnostic conventional coronary angiography (CCA), and to compare the biological effects with the estimated radiation dose as determined by established conversion factors in a randomized trial.
"The patients in our study were referred for suspected cardiac disease and were either randomized to CT or conventional angiography," Geisel said. After exclusion for recent exposure to ionizing radiation, 33 patients (median age, 62.3 years) underwent either 320-detector-row cardiac CT (n = 17) or conventional coronary angiography (n = 16). Blood samples were collected immediately before imaging, and again 60 minutes and 24 hours after each coronary imaging test. The study team then isolated the lymphocytes, stained the samples against the phosphorylated histone variant γH2AX, and counted the DSBs using fluorescence microscopy.
Prospective triggering on the 320-detector-row scanner (Aquilion One, Toshiba Medical Systems, Otawara, Japan) was set at 70% to 100% of the RR interval for heart rates 65 beats per minute (bpm) or less, and at 35% to 100% for patients with heart rates exceeding 65 bpm. The target rate of 65 bpm or less was reached for 14 of 17 coronary CTA patients. The imaging protocol included a scout image, a coronary artery calcium scan, and, finally, coronary CTA using bolus tracking. Conventional angiography was performed using the Judkins technique on an Axiom Artis DC imaging system (Siemens Healthcare, Erlangen, Germany).
The effective radiation doses were calculated using a conversion factor of 0.014 mSv per mGy per cm for CT and 0.22 mSv per Gy-cm2 for coronary angiography. Two patients requiring interventions during CCA were excluded to obtain comparisons for diagnostic tests only, leaving a total of 31 patients for analysis. "You can see a much higher DSB [for conventional angiography] than the higher dose may have suggested," Geisel said.
The results showed far less DNA damage for the low-dose coronary CTA exams compared to conventional angiography. After subtracting the baseline DSB count from the postimaging results, the researchers found an average of 0.11 ± 0.06 induced DSBs per cell for CTA and 0.31 ± 0.16 for conventional angiography. There was no significant difference between the baseline DSB value and the 24-hour value, demonstrating the rapid repair of DNA exposed to ionizing radiation.
Notably, the relative biological effect of conventional angiography was 1.89 ± 1.75 times higher (p < 0.001) than the corresponding estimated radiation doses (7.4 ± 4.1 mSv for conventional angiography and 4.9 ± 2.4 mSv for CT). There was excellent correlation between the measured biological effects and the estimated radiation doses for CTA (r = 0.992, p < 0.001) and moderate-to-good correlation for conventional angiography (r = 0.871, p < 0.001), Geisel said.
"We summarize that 320-detector-row cardiac CT leads to significantly fewer DNA double-strand breaks than diagnostic coronary angiography," he said. "This suggests that a conversion factor for the effective dose of coronary angiography may not be appropriate as it underestimates the biological effects."
A member of the audience commented that although the DSB comparisons are valid, conversion factors are inadequate for estimating the effects of the two different exams unless the cohorts are carefully matched.
By Eric Barnes
AuntMinnie.com staff writer
November 29, 2010
Related Reading
Less DNA damage seen after high-pitch coronary CTA, April 9, 2010
Firm promotes BioShield pill to address dose dilemma, September 15, 2009
Biological dose measures promise new view of cardiac imaging risk, May 1, 2009
Bisphosphonates may prevent radiation-induced leukemia, April 21, 2009
Researchers find genes that affect radiation damage, April 9, 2009
Copyright © 2010 AuntMinnie.com