Researchers from Johns Hopkins University have developed a PET radiopharmaceutical for imaging metastatic prostate cancer that so far has shown superior image quality with less radiation exposure in most radiosensitive organs than its predecessor.
The first human study of the agent, F-18 DCFPyL, was published online April 21 in Molecular Imaging and Biology. The researchers found that the small-molecule prostate-specific membrane antigen (PSMA) inhibitor caused no serious adverse events.
DCFPyL showed so much promise in preclinical studies that word about it is starting to spread, according to its developer and senior study author Dr. Martin Pomper, PhD.
 Dr. Martin Pomper, PhD, from Johns Hopkins.
Dr. Martin Pomper, PhD, from Johns Hopkins."Now I have people all over the country who are trying to come here to get scanned with this agent," he said.
Second-generation PET tracer
Before DCFPyL, Pomper and colleagues tested a first-generation agent known as F-18 DCFBC, which also binds to PSMA.
While DCFBC provided reliable detection of lesions, it also showed considerable blood-pool activity, which potentially could interfere with the detection of lymph-node metastases in the retroperitoneum and pelvis that are adjacent to large blood vessels, according to the authors.
To address the issue, Pomper and colleagues developed DCFPyL, which has also shown more than five times the tissue binding affinity for PSMA, compared with DCFBC, they wrote.
DCFPyL has a "better signal-to-noise ratio, so it is more sensitive than DCFBC, and DCFPyL has less radioactivity present in the blood, so you don't get all that background from the blood like you do with DCFBC ... [and you get] superior image quality," Pomper told AuntMinnie.com.
High-risk patients
In the current study, nine patients were referred for the scan by their physicians. The subjects had an average age of 70 years (range, 63-79 years) and an average weight of 82 kg (range, 79-84 kg). The Gleason score at first diagnosis was 7 for four patients, 9 for four others, and 10 in one case. Gleason scores are based on a scale of 2 to 10, with 10 representing the greatest likelihood that a cancer will spread.
"We are targeting patients who are at high risk of developing metastatic prostate cancer," Pomper said. "We are also targeting patients who have biochemical recurrence of the prostate cancer."
The subjects fasted for four to six hours before DCFPyL injection, which is the standard protocol for imaging with FDG at Johns Hopkins. A protocol of whether to fast prior to DCFPyL has not yet been established, the authors noted.
PET/CT scans (Discovery RX, GE Healthcare) were performed in 3D acquisition mode using CT for attenuation correction. A low-dose CT scan was performed prior to four sequential PET scans from the midthigh to the skull vertex beginning immediately after radiotracer injection.
No adverse events
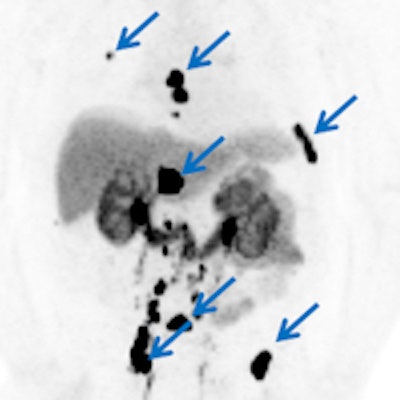
The researchers found "rapid" and "very high" accumulation of DCFPyL in putative foci of prostate cancer, with some lesions demonstrating maximum standardized uptake values (SUVmax) greater than 100.
 DCFPyL enhances the visual conspicuity of suspected sites (arrows) of metastatic prostate cancer. Image courtesy of Dr. Martin Pomper, PhD.
DCFPyL enhances the visual conspicuity of suspected sites (arrows) of metastatic prostate cancer. Image courtesy of Dr. Martin Pomper, PhD."These exceptionally high SUVmax numbers are comparable to the uptake reported in some metastatic prostate cancer sites evaluated with gallium-68-labeled PSMA-targeted ligands," they wrote.
In addition, areas of accumulation matched the researchers expectations, based on the known distribution of PSMA. For example, uptake was high in the salivary glands, probably reflecting their high density of PSMA, as well as in the kidneys. No radiotracer signal was found in the brain.
Compared with the previous research on DCFBC, there were significantly lower doses of DCFPyL in most radiosensitive organs, such as the thymus, osteogenic cells, red marrow, breasts, testes, uterus, and ovaries, as well as in other organs.
(Pomper and colleagues noted that they included radiation dose calculations for the breast, uterus, and ovaries to extend the findings, as they plan to explore applications for the radiotracer outside of prostate cancer.)
The low blood-pool activity of DCFPyL also allowed for higher lesion conspicuity compared to DCFBC, they wrote.
There were no reports of any severe adverse events among the nine subjects. One patient had a mild headache and nose bleed, but the researchers concluded that DCFPyL was likely not the cause. One other patient had a decreased platelet count, which was attributed to the initiation of prostate cancer treatment.
Pomper and colleagues now plan to expand the use of DCFPyL among prostate cancer patients and assess its potential with other types of cancer.
"We are working very closely with urologists who are determining what the best uses of this compound are," he said. "We are also going to use the agent to study antigen signaling in prostate cancer. And we are going to use it for image-guided therapy and for other cancers outside of the prostate."



















