Basing a decision to biopsy a thyroid nodule on the presence of certain ultrasound imaging characteristics could reduce unnecessary biopsies by 90%, according to a large study published online August 26 in JAMA Internal Medicine.
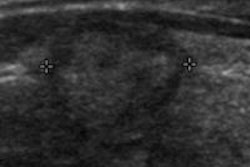
In the five-year retrospective study, which included thyroid cancer patients linked with the California Cancer Registry, a team of researchers led by Dr. Rebecca Smith-Bindman of the University of California, San Francisco (UCSF) found that three ultrasound nodule characteristics were associated with thyroid cancer:
- Microcalcifications
- Size greater than 2 cm
- Entirely solid composition
Requiring two of these characteristics to be present for a biopsy to be performed would dramatically reduce the number of unnecessary biopsies without missing many cancers, according to the group.
"If we restrict biopsy to those nodules that either have microcalcifications or are entirely solid and larger than 2 cm, we will find most cancers, and in patients in whom we don't biopsy, the risk of cancer is quite low (< 0.5 per 100)," Smith-Bindman told AuntMinnie.com. "This simple interpretation scheme can thus reduce surveillance and biopsies."
Practice variation
As a clinical radiologist who performs a lot of thyroid ultrasound, Smith-Bindman was struck by the dramatic variation in clinical practice, even within her own small group of ultrasound physicians, regarding who chose to perform biopsies on which lesions. In addition, none of the guidelines she found were evidence-based.
"An increasingly large number of patients were being referred for thyroid ultrasound because of incidental nodules seen on other imaging tests, and I realized I had no idea how common nodules were or their risk," she said. "So the project was motivated by a desire to improve clinical practice."
The UCSF team retrospectively studied 8,806 consecutive patients from January 1, 2000, to March 30, 2005, who underwent 11,618 thyroid ultrasound examinations. The researchers excluded patients if they had a prior unilateral or bilateral thyroidectomy for benign or malignant disease.
 Dr. Rebecca Smith-Bindman of the University of California, San Francisco.
Dr. Rebecca Smith-Bindman of the University of California, San Francisco.Of these patients, 105 were subsequently diagnosed as having thyroid cancer. The cancers in the cohort were determined through linkage with the California Cancer Registry, a population-based cancer registry in California (JAMA Intern Med, August 26, 2013).
To allow for a minimum of two years of follow-up, thyroid cancers were included in the study if they were identified through March 30, 2007. Those diagnosed as having nonthyroid malignant neoplasms (other than skin cancer) were excluded.
The group then matched all patients diagnosed with cancer with a control sample of patients without cancer on the basis of age, sex, and year of ultrasound examination.
The team retrieved the ultrasound exams of 96 cancer patients (91.4%) from the institution's PACS, as well as 369 control subjects. Each of these studies was reviewed independently by two board-certified radiologists, who were blinded to the cancer status. Any disagreements were resolved by consensus.
In 43 cancer patients (44.8%), ultrasound identified a single nodule, which was considered to be malignant. Multiple thyroid nodules were identified in 50 cancer patients (52.1%), while no nodules larger than 5 mm were identified on ultrasound in three patients (3.1%).
The final control group (515) was created from benign nodules in cancer patients (87) and nodules in patients never diagnosed as having thyroid cancer (428).
The researchers found that thyroid nodules were common among patients diagnosed with thyroid cancer (96.9%) and in patients not diagnosed with thyroid cancer (56.4%). The 96 cancer patients had 102 malignant nodules and 87 benign nodules.
Ultrasound characteristics
Only three ultrasound nodule characteristics were significantly associated with the risk of thyroid cancer:
- Microcalcifications (odds ratio [OR], 8.1; 95% CI: 3.8-17.3)
- Nodule size greater than 2 cm (OR, 3.6; 95% CI: 1.7-7.6)
- An entirely solid composition (OR, 4.0; 95% CI: 1.7-9.2)
The researchers then analyzed how these definitions of an abnormal ultrasound study would fare if they were used as an indication for nodule biopsy.
| Predictive value of proposed biopsy criteria | ||||
| Biopsy indication | Sensitivity | False-positive rate | Positive likelihood ratio | No. of biopsies performed per cancer detected |
| Presence of 1 US nodule characteristic | 0.80 | 0.44 | 2.0 | 56 |
| Presence of 2 US nodule characteristics | 0.52 | 0.07 | 7.1 | 16 |
While most cases of thyroid cancer would be detected if one characteristic was used as an indication for biopsy, this protocol would come with a high false-positive rate and a low positive likelihood ratio, according to the researchers. Fifty-six biopsies would be performed per cancer diagnosed.
Sensitivity (and false-positive rates) would be lower if two characteristics were required, but the positive likelihood ratio would be higher and only 16 biopsies would be performed per cancer diagnosed, according to the authors.
"Compared with performing biopsy of all thyroid nodules larger than 5 mm, adoption of this more stringent rule requiring two abnormal nodule characteristics to prompt biopsy would reduce unnecessary biopsies by 90% while maintaining a low risk of cancer (five per 1,000 patients for whom biopsy is deferred)," the authors wrote.
Good prognosis
Symptomatic thyroid cancer is rare, Smith-Bindman noted.
"Most thyroid nodules are benign and do not need biopsy or surveillance," she said. "Over 98% of thyroid nodules are benign."
Even for those with thyroid cancer, most have a favorable prognosis, with a 20-year survival rate greater than 97% even in patients who do not receive immediate treatment.
"Given the favorable prognosis of most thyroid cancers even without treatment, a risk of cancer of 0.5% among those with a negative examination result seems to balance between detection and unnecessary tissue sampling," the authors wrote. "Ongoing ultrasound imaging surveillance of patients with nodules who do not meet the criteria for biopsy is unlikely to prove beneficial given that our results ascribe these patients a low risk of cancer for as long as 10 years after imaging."
The researchers observed that the increased use and improved technical quality of ultrasound has led to detection of multiple morphologic characteristics, without clear criteria for what nodules need further treatment. This results in greater tissue sampling and excessive treatment, according to the group.
In mammography, the adoption of BI-RADS has been useful in facilitating comparative effectiveness work in breast imaging and efforts to standardize mammogram interpretation, the authors observed.
"Similar adoption of uniform standards for the interpretation of thyroid sonograms would be a first step toward standardizing the diagnosis and treatment of thyroid cancer and limiting unnecessary diagnostic testing and treatment," they concluded.