Flexible metallic stenting of the colon is common in patients treated for occlusive colorectal cancers. But conventional colonoscopy isn't a good way to follow up on these patients postoperatively, say Korean researchers who performed virtual colonoscopy (also known as CT colonography or CTC) on successfully stented patients soon after surgery.
For these patients, "colonoscopy is possible but may cause long-term damage to the scope" -- and to the stent itself -- according to Dr. Seong Ho Park from Asan Medical Center in Seoul, South Korea. Stented patients need follow-up due to a "high risk of synchronous cancers," but no previous studies had been performed in such a cohort, he said.
The investigators performed the study to evaluate the feasibility of CTC for examining the proximal colon after flexible metallic stent placement for acute malignant colonic obstruction. They presented their results at the 2009 International Symposium on Virtual Colonoscopy in Reston, VA.
All 51 patients in the retrospective study (34 men, 17 women; mean age, 58.3 ± 7 years) had been stented successfully for occlusive cancer without complications within the previous one to 43 days (median, five days).
Conventional colonoscopy had failed to advance past the stent in five patients; CTC was the initial referral for the other 46, Park said. Virtual colonoscopy was performed after cathartic bowel preparation using magnesium citrate (n = 24) combined with oral bisacodyl, or polyethylene glycol (n = 27).
 |
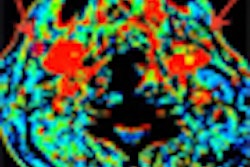
| CTC was successful in a 58-year-old woman with a flexible metal stent in the rectosigmoid junction. All images courtesy of Dr. Seong Ho Park. |
Due to the high risk of perforation in the postoperative patient cohort, only iodine (diatrizoate 100 mL) was used for tagging, and the patients also underwent a "low-dose baseline exam" (120 kVp, 20 mAs, 5-mm collimation) before the full prone and supine image acquisition, Park said. "We wanted to exclude perforation before insufflation."
At this stage, one patient was excluded for occult colonic perforation, leaving 50 for analysis.
The remaining 50 patients underwent automated CO2 insufflation (ProtoCO2l, Bracco Imaging, Milan, Italy) followed by prone and supine CT image acquisition (120 kVp, 50 mAs) at 1-mm collimation, with slices reconstructed at 0.7-mm increments.
 |
| CTC was successful in a 51-year-old patient with a stent in the rectosigmoid junction. CTC detected a 15-mm synchronous cancer in the ascending colon. Stent can be seen in the rectosigmoid junction. |
The reference standard for the findings included surgical specimens and/or postsurgical colonoscopy with lesion matching (i.e., within one segment and within 50% of size) as well as CTC findings and clinical observations, Park said.
Interpreting the results on a 3D Rapidia virtual colonoscopy workstation (Infinitt, Seoul, South Korea), the group assessed exam quality and rated the findings using C-RADS reporting. Lesions 6 mm and larger were reported, as well as stent dislodgment/migration, extraluminal air, and any contrast spillage. Six percent of the studies were technically inadequate owing to noncompliance with the tagging regimen and, in one case, inadequate distention.
"Virtual colonoscopy was performed successfully in all five patients with prior failed colonoscopy due to the stent," Park said.
Per-lesion sensitivity for lesions 6 mm and larger in the proximal colon was 85.7% (12 of 14 lesions). Both synchronous cancers and all five advanced adenomas were also found. Overall, seven of nine adenomas were found -- an 8-mm and a 6-mm sessile adenoma were missed. Per-patient sensitivity was 90% (nine of 10 patients), Park said.
 |
 |
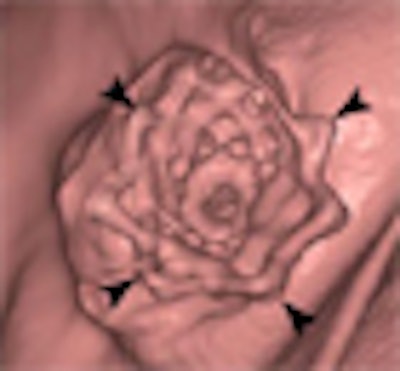
| CTC was successful in this patient, but a synchronous 8-mm tubular adenoma was missed. Stent can be seen in the rectosigmoid junction. |
For lesions 6 mm and larger in the proximal colon, per-patient specificity was 85.7% (18 of 21 patients; 95% confidence interval: 64.5%-95.9%). There were no CTC-related complications in the 50 patients. There were three false positives (two 6-mm polyps and one 8-mm polyp) but no erroneous changes in surgical planning, he said. Finally, there were no perforations and no stent dislodgement or migration.
"The same methods used for CTC in other lesions can be performed after colon stenting," Park said. "CTC is an effective examination for proximal colon evaluation after metallic stent placement for acute malignant colonic obstruction."
By Eric Barnes
AuntMinnie.com staff writer
January 27, 2010
Related Reading
MR colonography separates benign from malignant colonic strictures, January 16, 2009
Swiss study links prostate radiotherapy to higher colon cancer risk, June 24, 2008
VC with automated insufflation effective in stenosing cancer, March 24, 2008
Patients show slight preference for MR colonography over colonoscopy, June 6, 2007
MR colonography disappoints in reduced-prep protocol, March 6, 2007
Copyright © 2010 AuntMinnie.com