A once-common surgical technique that's fallen out of favor has left a few patients with false-positive virtual colonoscopy findings.
A recent American Journal of Roentgenology paper reveals the possibility of mistaking an appendiceal stump for a clinically significant colorectal polyp. If misdiagnosed on VC, the patient could be sent for same-day colonoscopy, adding needless risk and costs to colorectal cancer screening.
The finding of a polypoid or mass lesion at the cecal tip after an appendectomy has been previously described at optical colonoscopy and barium enema examination, the authors noted.
"Historically, the technique of inversion-ligation appendectomy was used by some surgeons to theoretically reduce the risk of peritoneal contamination in the setting of acute appendicitis," wrote Drs. Tyler Prout, Andrew Taylor, and Perry Pickhardt from the University of Wisconsin Medical School (American Journal of Roentgenology, February 2006, Vol. 186:2, pp. 535-538).
"This technique has also been used for incidental appendectomy performed during laparotomy for unrelated problems," they wrote. "The resultant appendiceal stump usually necroses and sloughs into the colonic lumen after several days, but remnant tissue may persist in some patients."
A recent review of this surgical technique concluded that the additional step of stump inversion is not necessary, but patients with a history of appendectomy continue to present with the equivocal findings, they wrote.
The paper presents two cases in which an appendiceal stump simulated a large pedunculated polyp in asymptomatic adults undergoing screening virtual colonoscopy.
"In a patient with a prior appendectomy, the specific location and appearance of this entity at CTC (CT colonography, or VC) may be sufficient for diagnosis, but the possibility of a significant neoplasm may be difficult to exclude in some cases," the Wisconsin group wrote.
 |
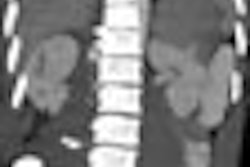
| Inverted appendiceal stump in 63-year-old asymptomatic woman referred to CT colonography (CTC) for routine colorectal cancer screening. Three-dimensional endoluminal view from prone CTC dataset shows discrete 10-mm pedunculated polypoid lesion located at medial aspect of cecal tip. Image republished with permission of the American Roentgen Ray Society (AJR 2006; 186:535-538). |
 |
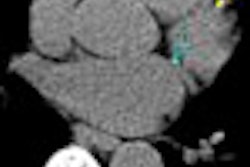
| Inverted appendiceal stump in 63-year-old asymptomatic woman. Prone transverse (B) 2D images from CTC confirm pedunculated lesion (arrow) detected on 3D view and show its soft-tissue composition. Lesion is located at or near appendectomy site, but this does not completely exclude possibility of neoplasm. Image republished with permission of the American Roentgen Ray Society (AJR 2006; 186:535-538). |
 |
| Inverted appendiceal stump in 63-year-old asymptomatic woman. Coronal (C) 2D images from CTC confirm pedunculated lesion (arrow) detected on 3D view and show its soft-tissue composition. Image republished with permission of the American Roentgen Ray Society (AJR 2006; 186:535-538). |
The patient described above was referred for routine colorectal screening with VC. Her surgical history was significant only for remote appendectomy. She underwent standard bowel preparation of oral sodium phosphate (45 mL), 2% barium sulfate suspension (250 mL), and water-soluble iodinated contrast material (diatrizoate, 60 mL) the day before the exam.
Supine and prone CT images were acquired on a MDCT scanner (LightSpeed Ultra, GE Healthcare, Chalfont St. Giles, U.K.) using an 8 x 1.25 detector configuration, 1-mm reconstruction interval, 120 kVp, and 50 mAs. The study was interpreted by an experienced gastrointestinal radiologist using V3D Colon software (Viatronix, Stony Brook, NY). Primary 3D interpretation with 2D correlation of suspicious findings was used to interpret the results.
CT findings revealed a 10-mm pedunculated polypoid lesion at the medial base of the cecum. No additional findings were identified, but despite the surgical history and location of the lesion, "a neoplastic polyp could not be confidently excluded," the authors wrote. The patient was referred for conventional colonoscopy, which was negative.
"The endoscopic appearance of the polypoid cecal lesion was thought to be most compatible with an inverted appendiceal stump," the authors wrote. Biopsies revealed benign colonic mucosa with underlying lymphoid tissue.
The second report was of a 58-year-old asymptomatic woman with a history of appendectomy. Routine screening VC showed a large pedunculated polypoid lesion in the cecum that demonstrated a subtle focus of internal fat attenuation on the 2D images.
"An inverted stump was prospectively suggested, but the patient still went on to same-day optical colonoscopy because a significant neoplasm could not be absolutely excluded."
The polyp was confirmed and removed at endoscopy and the polyp site cauterized, the radiologists wrote. "Although not suspected at optical colonoscopy, at pathologic evaluation the lesion was found to be an appendiceal stump."
The location and appearance of an appendiceal stump "generally allow its recognition at VC, but in some cases the possibility of a significant neoplasm cannot be completely excluded," the group concluded.
By Eric Barnes
AuntMinnie.com staff writer
March 1, 2006
Related Reading
Diverticular disease doesn't impede VC in Wisconsin study, November 28, 2005
VC practice thrives in Wisconsin, May 5, 2005
HMO pays for screening virtual colonoscopy, June 4, 2004
VC fares better as its own gold standard, September 8, 2004
Group credits 3D reading for best-ever VC results, October 15, 2003
Copyright © 2006 AuntMinnie.com