Introduction
The correct diagnosis of shoulder pathology, such as rotator cuff tears, is important but can be challenging. Ultrasound allows presentation of the soft-tissue structures and some parts of the cartilage. A review of published literature on this subject indicates a wide range of sensitivities (57% to 100%) and specificities (50% to 100%) in detecting rotator cuff tears and other shoulder pathologies (6, 14). The sonographic criteria used, the patient population examined, the diagnostic information required, and operator dependency are all crucial factors in explaining this wide range of results.
Shoulder sonography protocols have been revised in recent years, resulting in more accurate examinations. In the rotator cuff, for example, techniques have been refined for improved visualization. The use of high-resolution linear-array transducers, tissue harmonic imaging (THI), extended field-of-view techniques and 3D ultrasound are just some of the advances.
One of the main advantages of 3D US is its multiplanar imaging capability, which can represent the shoulder simultaneously in three perpendicular orthogonal planes. Unlike 2D US, 3D US provides the extra coronal view, allowing a complete appreciation of the full extent of rotator cuff tears, and 3D reconstruction permits a comprehensive pictorial of the tears. Recent studies indicate that ultrasound is as accurate as MRI for detecting rotator cuff tears (click here for references).
This pictorial presentation outlines our initial experiences with 3D US in patients who visited the Studio Ecograficao Dott. Stefano Ciatti in Prato, Italy, for shoulder sonography. These patients are part of a larger study that we are currently conducting that will evaluate the use of 3D US combined with 2D US for detecting rotator cuff tears and other shoulder pathologies.
Materials and methods
Since 2000, 558 patients have visited our institute for sonographic examination of the shoulder. These patients have had one or both shoulders examined with a combination of 2D US and 3D US.
Shoulder examinations were initially performed on the Kretz 530 MD ultrasound system with a 6- to 12-MHz linear-array transducer. We now work with a Voluson 730 Expert system (GE Healthcare, Chalfont St. Giles, U.K.), which also has a 6- to 12-MHz linear-array transducer. The latter permits scanning with 2D and 3D automatic volume acquisition.
Our examination technique involves scanning the rotator cuff tendons individually with real-time 2D US followed by 3D US. The duration of the volume acquisition may vary depending on the width of the volume (ranging from 15° to 29°) and the size of the volume box defining the region of interest.
On average, a volume acquisition in shoulder sonography requires approximately seven seconds. Once the volume data has been obtained, the patient can relax the arm (often much appreciated if he or she is in pain). In the meantime, the acquired volume is studied in the longitudinal, transverse, and coronal planes, and 3D reconstruction is performed when necessary.
Shoulder pathology
Tendinopathy and tendinitis
 |
| 3D US and multiplanar imaging of the subscapularis tendon of the rotator cuff in a patient suffering from tendinitis. All three planes show signs of tendon irregularity, enlargement, and dishomogeneity. Multiple focal calcifications are seen in all planes throughout the entire tendon fibers. The use of 3D reconstruction of the same subscapularis tendon demonstrates more clearly the full extent of focal calcifications, tendon irregularity and enlargement, and tendon dishomogeneity. All images courtesy of Dearbhla O'Dwyer and Dr. Stefano Ciatti. |
 |
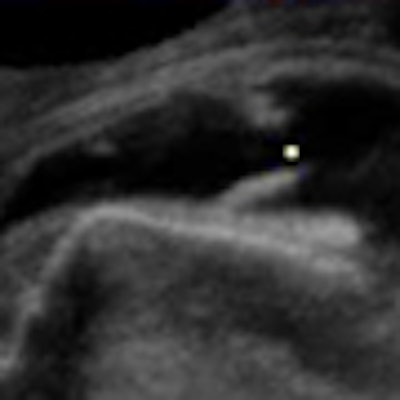
| Multiplanar localization of a large calcific deposit at the insertion of the rotator cuff demonstrating posterior acoustic shadowing on the transverse and longitudinal planes. The coronal plane demonstrates the full size and extension of this calcific deposit within the fibers of the tendon. 3D US provides the opportunity to accurately pinpoint these calcifications and ensure that the needle is placed in the correct position to perform needle aspiration of these calcific deposits. |
 |
| Multiplanar and 3D representation of biceps tendinitis in a patient suffering from shoulder pain and weakness. Note the focal calcifications at the level of the insertion, enlarged and irregular biceps tendon, and effusion. |
 |
| 3D reconstruction with surface rendering of the long head of the biceps tendon with three macrocalcifications seen to the left side of the untorn tendon in a patient with tendinitis. |
Rotator cuff tears
Rotator cuff tears are characterized by their size, location, and degree of the tear (partial- or full-thickness tear). Traditionally, the width and location of a tear is evaluated using transverse views; longitudinal views assist in evaluating the degree of retraction from the greater tuberosity.
3D US presents the anatomy of interest in longitudinal, transverse, and coronal planes. Having an extra plane with which to view the tear of a particular tendon is extremely useful in determining if a tendon has a full- or partial-thickness tear.
Shoulder sonography using 3D US in all orthogonal planes allows more accurate estimation of the cross-sectional area, depth, and location of a tear. The coronal plane gives a direct frontal view of any tendon being examined and permits clear visualization of a tear and its extent. The coronal plane also clearly shows if intact tendon fibers remain or the tendon has completely ruptured. The use of the coronal view with 3D surface-rendered images permits a better understanding of the condition of the remaining free, frayed edges.
The quality of the tendon ends and the full extent of the tears are useful information for the orthopedic team when surgical intervention is planned. Multiplanar and 3D-rendered images are better understood by the orthopedic surgeon.
 |
| Multiplanar representation of a subscapularis tendon partial tear. All three planes demonstrate an area of an irregular anechoic defect in the upper surface of the tendon (on the bursal side of the rotator cuff) while inferiorly, the tendon remains intact. |
 |
| Multiplanar representation of a massive tear (more than 5 cm and involving more than one tendon) of the rotator cuff. |
Biceps tendon
Evaluating the biceps tendon is essential when searching for a rotator cuff tear. Frequently, abnormalities of both structures coexist. Clinically, biceps tendon lesions can simulate rotator cuff pathology.
Bicipital tendinitis is present in almost all patients with a rotator cuff defect. The most important associated abnormality is an effusion within the biceps tendon sheath usually seen inferior to the tendon groove where the sheath expands to accommodate the fluid.
 |
| Biceps tendinitis associated with rotator cuff defect. The coronal plane readily demonstrates subtle tears and irregularities of the biceps tendon within an effusion. 3D reconstruction confirms the irregularities of this tendon and the large effusion is well-appreciated. Bottom right image demonstrates fluid collection and right coracobrachialis longus (CBL). |
 |
| Multiplanar and 3D imaging of a completely ruptured biceps tendon. This is a study of an elderly patient who, after having lifted a heavy load, presented with weakness of the arm and swelling at the level of the middle of the humerus. One must follow the length of the biceps tendon from its origin to its insertion with the muscle. With acute traumatic rupture of the biceps tendon, the muscle contracts and collapses upon itself distally while the tendon retracts as in the above case. All planes demonstrate a fluid collection within the biceps sheath, the absence of any tendon fibers throughout the fluid collection, and the collapsed biceps muscle beneath. |
Partial tear
The biceps tendon may have a partial tear, either horizontally or longitudinally. Be sure that the second structure is a part of the biceps tendon and not a loose body within the tendon sheath, giving the appearance of the second tendon in cross-section.
 |
| A lengthways split results in two cords, giving the appearance of two tendons lying side by side over a variable length of the tendon, as may be seen in the multiplanar images above. |
 |
| This 3D reconstruction confirms the existence of a lengthways split within the biceps tendon. Two cords are seen lying parallel within the bicipital groove. |
 |
| Multiplanar demonstration of a post-traumatic partial tear on the bursal aspect of the rotator cuff (infraspinatus tendon). The coronal plane and 3D reconstruction demonstrate dramatically the full extent of this tendon tear (indicated by the arrows), which initially on the transverse and longitudinal planes seems less extensive. |
 |
| Multiplanar imaging, including 3D reconstruction, of a torn supraspinatus tendon with underlying tendinitis (with no history of trauma). Lower right, note the focal calcification at the insertion of the tendon into the greater tuberosity and smaller calcifications throughout the tendon. The intact portion of the remaining tendon is demonstrated beside the anechoic fluid-filled space where the tendon has broken. The free, frayed edges of the tendon are clearly visible. |
 |
| Above, 3D reconstruction of the infraspinatus tendon with both insertional and intrasubstance tears in an elderly patient who fell and hit his shoulder. Below, multiplanar representation of a large hematoma in the same patient who is under anticoagulant therapy. The coronal plane allows correct measurement of the hematoma. |
 |
 |
| 3D reconstruction with surface-rendering of a supraspinatus tendon clearly demonstrating a tear and the free, frayed edges. Note also the remaining tendon fibers intact. |
 |
| Above and below, post-traumatic multiplanar and enlarged 3D reconstruction of the supraspinatus tendon with small marginal tears that were better depicted using 3D reconstruction. |
 |
 |
| 3D representation of a post-traumatic rupture of the supraspinatus tendon. |
Conclusion
3D sonography improves visualization of joint anatomy by providing a single, integrated view of the entire structure, offering a more complete and comprehensive understanding of the anatomic and spatial relationships. 3D ultrasound permits images to be cross-referenced to one another simultaneously, and a single 3D US acquisition can obtain the standard images that are required to evaluate anatomy. Images also can be obtained in the coronal plane, resulting in a frontal image that is unavailable with 2D US.
In addition, 3D US reconstruction frequently produces images that are better appreciated by surgeons and patients. Advanced technology, such as volume rendering and rotation, allow for interactive manipulation of volume data. The integration of views permits better visualization and allows for a more accurate diagnosis.
In our experience, automatic volume acquisition offers a valuable tool to evaluate tendons and muscles, allowing us to decide on how to proceed with the exam. Applied to shoulder sonography, this means a more precise evaluation of the size and extent of rotator cuff tears.
Finally, 3D US is a patient-friendly modality, especially if the person is in a great deal of pain. The patient's arm only has to be positioned once as the volume acquisition data is obtained. Once the data is gathered, the patient can relax while the data is manipulated. High-quality images are obtained with minimal discomfort to the patient.
By Dearbhla O'Dwyer and Dr. Stefano Ciatti
AuntMinnie.com contributing writers
March 21, 2008
Sonographer Dearbhla O'Dwyer, B.Rad, H.Dip D.I.(U/S), and Dr. Stefano Ciatti are in private practice at the Studio Ecograficao Dott. Stefano Ciatti in Prato, Italy.
Related Reading
US guidance needles away the pain of rotator cuff calcific tendinitis, November 29, 2007
Making the most of MRI to assess the rotator cuff pre- and postinjury, November 9, 2007
US shows full spectrum of shoulder injuries, September 26, 2006
References
Adler RS, "Future and new developments in musculoskeletal ultrasound" (Radiologic Clinics of North America, July 1999, Vol. 37:4, pp. 623-631).
Adler R, Fatchett J. "Enhanced 3D Reslice Clinical Case Study Report: Case studies using advanced 3D view reslice technology for detecting rotator cuff tear involvement of the shoulder."
American Institute of Ultrasound in Medicine, "Practice Guidline for the Performance of a Shoulder Ultrasound Examination (Journal of Ultrasound in Medicine, October 2003, Vol. 22:10, pp. 1137-1141).
Belli P, Costantini M, Mirk P, Leone A, Pastore G, Marano P, "Sonographic diagnosis of distal biceps tendon rupture: A prospective study of 25 cases" (Journal of Ultrasound in Medicine, June 2001, Vol. 20:6, pp. 587-595).
Bianchi S, Martinoli C, Bianchi-Zamorani M.P, Valle M, "Ultrasound of the joints" (European Radiology, January 2002, Vol. 12:1, pp. 44-55).
Brandt TD, Cardone BW, Grant TH, Post M, Weiss CA, "Rotator cuff sonography: a reassessment" (Radiology, November 1989, Vol. 173:2, pp. 323-327).
Burkhead W Jr., ed, Rotator Cuff Disorders, Lippincott, Williams & Wilkins, Philadelphia, 1996.
Farin PU, Jaroma H, "Acute traumatic tears of the rotator cuff: Value of sonography" (Radiology, October 1995, Vol. 197:1, pp. 269-273).
Hammar MV, Wintzell GB, Astrom KGO, Larsson S, Elvin A, "Role of US in the preoperative evaluation of patients with anterior shoulder instability" (Radiology, April 2001, Vol. 219:1, pp. 29-34).
Hunerbein M, Raschke M, Khodadadyan C, Hohenberger P, Haas N, Schlag P, "Three-dimensional ultrasonography of bone and soft tissue lesions" (European Journal of Ultrasound, April 2001, Vol. 13:1, pp.17-23).
Lin EC, Middleton WD, Teefey SA, "Extended field of view sonography in musculoskeletal imaging" (JUM, February 1999, Vol. 18:2, pp. 147-152).
Lin J, Fessell DP, Jacobson JA, Weadock WJ, Hayes CW, "An illustrated tutorial of musculoskeletal sonography: Part 1, Introduction and general principles" (American Journal of Roentgenology, September 2000, Vol. 175:3, pp. 637-645).
Mack LA, Matsen FA III, Kilcoyne RF, "US evaluation of the rotator cuff" (Radiology, October 1985, Vol. 157:1, pp. 205-209).
Martinoli C, Bianchi S, Dahmane M, Pugliese F, Bianchi-Zamorani MP, Valle M, "Ultrasound of tendons and nerves" (European Radiology, January 2002, Vol. 12:1, pp. 44-55).
Menias CO, Middleton WD, Teefey SA, "An overview of ultrasonography of the Shoulder" (Ultrasound Quarterly, 2000, Vol. 16:4, pp. 171-183).
Middleton WD, "Ultrasonography of the shoulder" (Radiologic Clinics of North America, September 1992, Vol. 30:5, pp. 927-940).
Miller TT, Adler RS, "Sonography of tears of the distal biceps tendon," (American Journal of Roentgenology, October 2000, Vol. 175:4, pp. 1081-1016).
Peetrons P, "Ultrasound of muscles" (European Radiology, January 2002, Vol. 12:1, pp. 35-43).
Rawool NM, "Ultrasound shows high sensitivity in rotator cuff" (Diagnostic Imaging, 2002, pp. 46-50).
Sanders R, Winters T, Clinical Sonography: A Practical Guide, 2nd ed., Lippincott, Williams & Wilkins, Philadelphia, 1991.
Sandrick K, "3-D Ultrasound" and "Sonography teams up with MRI in shoulder" (Diagnostic Imaging, 2001, pp. 51-56; Diagnostic Imaging, sports imaging supplement, September 2000, pp. 10-11).
Teefey SA, Middleton WD, Yamaguchi K, "Shoulder sonography. State of the art" (Radiologic Clinics of North America, July 1999, Vol. 37:4, pp. 767-785, ix).
Trentanni C, Ecografia Della Spalla, Athena Audiovisuals, 2001.
van Holsbeeck M, Introcaso J, eds., Musculoskeletal Ultrasound, 2nd ed, Elsevier, St. Louis, 2001.
Copyright © 2008 Dearbhla O'Dwyer and Dr. Stefano Ciatti