As many as half of all vertebroplasty patients wind up with a new compression fracture, most often in the adjacent vertebral bodies. The leaking of cement into the disk space can increase the risk of new fracture. But preoperative MR exams can help predict which patients are more likely to have cement leakage, according to a paper in the April American Journal of Roentgenology.
The study was conducted at the University of Rochester Medical Center in New York and was led by Dr. Akio Hiwatashi. Hiwatashi has since moved to Kyushu University in Fukuoka, Japan. His co-authors are from institutions in Rochester, as well as Tokyo and Osaka, Japan.
The patient population consisted of 46 people and 107 vertebral bodies with painful osteoporotic compression fractures, mostly at the thoracolumbar junction. Preoperative MR imaging was done on a 1.5-tesla scanner and the protocol included fast spin-echo sagittal T2-weighted imaging, sagittal spin-echo T1-weighted imaging, and a sagittal spin-echo, fat-suppressed contrast-enhanced T1-weighted sequence. Postvertebroplasty imaging was done with CT. The mean interval between MR imaging and treatment was seven days with all postsurgical CT performed within 24 hours.
 |
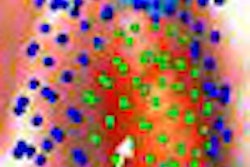
| A 68-year-old woman with history of long-term steroid use for chronic obstructive lung disease. Sagittal T2-weighted image before vertebroplasty shows compression fracture of T11 vertebral body with concave deformity. Cortical defect is noted in superior endplate (arrow). Hyperintensity is noted in adjacent desiccated intervertebral disks, which is more prominent at T10-T11 (arrowhead). |
 |
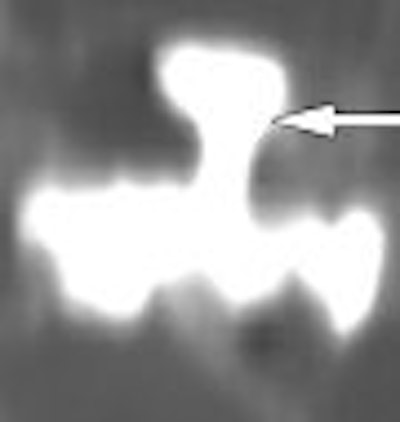
| Same patient as above. Sagittal reformatted CT image after vertebroplasty shows cement leakage in T10-T11 disk space (arrow) through cortical defect seen on preoperative MR image. Hiwatashi A, Ohgiya Y, Kakimoto N, Westesson P, "Cement Leakage During Vertebroplasty Can Be Predicted on Preoperative MRI" (AJR 2007; 188:1089-1093). |
"We defined a cortical defect as a discontinuation of cortical hypointensity on sagittal T2-weighted or fat-suppressed contrast-enhanced T1-weighted images," the authors explained (AJR, April 2007, Vol. 188:4, pp. 1089-1093).
According to the results, cement leakage into the adjacent disk during vertebroplasty occurred in 24% of 214 disk spaces. Leakage was associated with cortical defect in the endplate, abnormal T2-weighted hyperintensity in the adjacent vertebral disk, and the absence of intravertebral cleft. Cortical defect was seen in 33% of the endplates, and 65% of the cases had cement leakage.
"This study has shown that vertebral compression fracture with cortical defect and abnormal T2 high signal in the adjacent disk has an increased risk for cement leakage," the authors concluded. In an interesting aside, they noted less cement leakage in fractures with an intravertebral cleft, probably because there was less resistance in the cleft during cement injection.
At the 2006 RSNA meeting in Chicago, Hiwatashi said that seeing these MR changes should encourage physicians to change their vertebroplasty technique, such as the placement of the needles tips or by using a "stickier" cement formula. Pretreatment MR images can play a part in determining if a patient should have vertebroplasty or kyphoplasty, he said ("RSNA Daily Bulletin," November 27, 2006).
By Shalmali Pal
AuntMinnie.com staff writer
April 3, 2007
Related Reading
Vertebroplasty increases vertebral height, imaging shows, May 2, 2006
New fractures occur sooner in adjacent vertebrae following vertebroplasty, January 24, 2006
Bone marrow edema on preop MR correlates with vertebroplasty success, May 18, 2006
Copyright © 2007 AuntMinnie.com