By Dr. George Koulouris
At the 2001 RSNA meeting in Chicago, Dr. George Koulouris from the Victoria House Private Hospital in Melbourne, Australia shared his group’s research on the value of MRI for hamstring injuries. Soon after, the team received a research grant from the Australian Football League to further study acute injuries to the hamstring muscle complex. In this article, Dr. Koulouris discusses this work in progress.
The aim of this research is to obtain a prospective comparative analysis of the main imaging modalities -- MRI and ultrasound -- used to investigate strain to the hamstring muscle complex (HMC) with clinical assessment, and to determine which of the three is the most accurate at predicting return to competition.
The study sample thus far consists of 65 professional players from the Australian Football League, with a total of 80 to be investigated. Australian Rules Football (AFL) is a unique sport, which is characterized by prolonged aerobic activity with intense bursts of anaerobic exercise. As it involves kicking and ballistic movements, the sport lends itself to high rates of hamstring injury, making it the leading cause of missed games (AFL Injury Report Survey, 1992-2000).
 |
| Hyperintensity of the proximal portion of the long head of biceps femoris muscle is compatible with a strain (arrow). |
Repeated imaging and clinical examinations are performed at the time of initial presentation, as well as at two and six weeks post-injury. Outcomes of return to training and finally competition, as well as any indicators that may usefully predict risk of re-injury, are important parameters currently under investigation.
 |
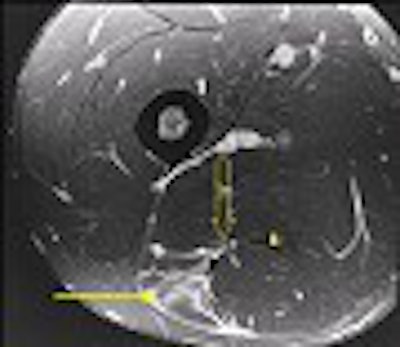
| Axial images of the same patient as above demonstrate again the tear at the musculotendinous junction (arrow). Further to this, a rim of hyperintensity is noted around the fascial layer of the muscle boundary (arrowheads). The sciatic nerve is identified anterior to the muscle, however not in contact with the extravasated fluid (open arrow). The corresponding sonogram was also abnormal, with the player missing competition for three weeks. |
Our imaging protocols consist of the following: On a Signa Horizon MR/i l.5-tesla scanner (GE Medical Systems, Waukesha, WI): axial and coronal oblique inversion-recovery proton-density sequences, SHOPA phased-array coil (TR/TE 4000/43, 512 x 384, 3-mm slices, no gap). Sonography was done with an HDI 5000 super-premium general imaging scanner (Philips Medical Systems North America, Bothell, WA) with 5-12 MHz linear probe.
 |
| Axial MR images through another patient demonstrates a tear of the belly of semitendinosus (arrow) with the tendon also noted (arrow head). Free fluid around the muscle comes into contact with the sciatic nerve (open arrow) which accounted for the patients' clinical symptoms of radiculopathy. |
Though the data has not been collated and analyzed yet, we have found a high degree of correlation between the imaging modalities and clinical examination. Occasionally, discrepancies between all three have been observed (see Figures 1-5).
MR imaging is noted to be more sensitive in the detection of soft-tissue injury compared to ultrasound, particularly in the setting of edema without visible macroscopic disruption. MRI scans demonstrated edema and hemorrhage as bright signal on proton-density sequences, which acts as a direct contrast with the gray isointense signal of muscle. This accounts for the high sensitivity of this modality, as well as the benefits of multiplanar capability (also a benefit of sonography).
MRI also probably depicts fluid around the sciatic nerve more accurately, which may account for neural tension and radiculopathy following injury. This has been postulated to be a cause of recurrent injury following injury to the HMC, as well as a prolonged rehabilitation period.
So far, sonography has proved to be less than ideal for HMC imaging. The low echogenic signal of edema on the background of normal dark gray muscle on sonography is difficult to appreciate. In addition, sonography is disadvantaged by the fact that it is highly operator dependent.
 |
| A sonogram of the same patient examined above reveals a macroscopic tear (arrow) as evidenced by an area of low echogenicity with a degree of muscle retraction. The hypoechoic rim around this tear correlates with the surrounding fluid visualised on MR imaging (arrowheads). |
However, the advent of new high-frequency probes, and the advantage of clinical correlation with a cooperative patient, make it possible to provide a more focused and detailed examination. While this raises the sensitivity of sonography, it does not make it the gold standard for hamstring imaging.
 |
| Oblique coronal MR images demonstrate a classic musculotendinous junction tear of the biceps femoris muscle, displaying the characteristic feathered appearance. The corresponding sonogram was normal and a rapid return to competition was noted. Images courtesy of Dr. George Koulouris. |
We look forward to releasing our data as the study approaches completion, within the next 6-9 months. The information is expected to provide a better understanding of the role of imaging in this specific clinical setting, as well as the significance of abnormalities detected. This will assist the referring sports clinicians and orthopedic surgeons in rehabilitating elite athletes.
By Dr. George KoulourisAuntMinnie.com contributing writer
July 22, 2002
Related Reading
MRI spots hamstring injuries, keeps skaters flying high, February 25, 2002
MRI says it all for UU technologist, February 21, 2002
Stress fractures and spondylolysis plague serious skaters, February 20, 2002
Use of ultrasonographic guidance in interventional musculoskeletal procedures, April 13, 2001
Ultrasound wins the gold at Sydney, November 8, 2000
Copyright © 2002 AuntMinnie.com



















