Researchers from the University of Maryland in Baltimore have found that contrast-enhanced MRI and FDG-PET can help in the accurate differentiation between viable and nonviable myocardium in patients with implantable cardioverter-defibrillator (ICD) devices undergoing ventricular tachycardia ablations.
The group who produced the study, which was presented last week at the American Society of Nuclear Cardiology (ASNC) annual meeting, added that the additional information gathered from contrast-enhanced MR and FDG-PET images should help reduce procedure time and guide patient therapy.
The lead researcher of the study was Jing Tian, MD, PhD, a research associate in the University of Maryland's division of cardiology. The study was a collaboration between the university's department of medicine, division of cardiology, and department of diagnostic radiology and nuclear medicine
Sudden cardiac death
Ventricular tachycardia is a rapid beating of the heart or arrhythmia, which potentially can lead to sudden cardiac death. The condition is often due to scar tissue in the heart, which can be caused by myocardial infarction and/or coronary artery disease. This heterogeneous scar tissue consists of viable tunnels that pass through the tissue.
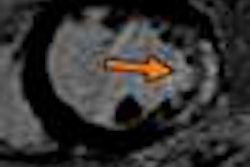
"Treatment of ventricular tachycardia [involves trying] to cauterize the heart tissue along the scar border, so that we can cut off the tunnels and hopefully terminate the abnormal circulation," Tian said. "That's why it is very important for us to know exactly the scar location, the size, and the geometry."
FDG-PET has been established for decades for defining viability of the myocardial tissue. "However, given the resolution of the FDG-PET imaging studies, about 6 mm is very challenging for this kind of modality to give us a very detailed border and geometry of the scar."
While nuclear medicine techniques, such as rubidium-82 and FDG-PET, currently are used to diagnose myocardial viability, the researchers noted that the modality does not allow for direct visualization of the 3D geometry of myocardial scarring.
MRI versus PET
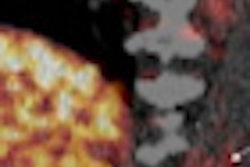
"If you think about the strengths and limitations of each modality, MRI's strength is to assess the transmurality of myocardiac injury and the strength of FDG-PET is to assess the metabolic activity at a cellular level, whether the cells within the injured myocardium are still viable," added senior study author Vasken Dilsizian, MD, chief of the division of nuclear medicine at the University of Maryland School of Medicine.
"While MRI will tell you which part of the myocardium is scarred and how extensive it is, because it does not interrogate myocardial cells, MRI cannot determine whether within those scar tissues there are viable cells that still use glucose metabolism which can be imaged with FDG-PET," he continued. "By combining the two [modalities], we are able to characterize the area of the scar and whether there is any viable FDG-using myocardial cells within or around the scar tissue."
The researchers evaluated 10 patients with ischemic and nonischemic cardiomyopathy, who received both contrast-enhanced MRI and FDG-PET scans prior to ventricular tachycardia ablation. The patients' hearts were divided into 17 segments, with a total of 93 segments analyzed. Segments with ICD artifacts were excluded.
Contrast-enhanced MRI segments demonstrating scar areas were further classified based on the relative amount of contrast enhancement per myocardial segment into groups as follows:
- Less than 25% contrast enhancement
- 25% to 75% contrast enhancement
- Greater than 75% contrast enhancement
The researchers used receiver operator characteristics (ROC) analysis to determine the MRI scar transmurality cutoff with the best sensitivity and specificity to differentiate viable and nonviable tissue via PET, with 50% FDG uptake as the median point to determine viability.
FDG uptake
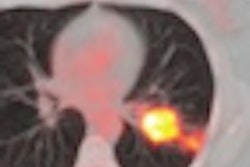
According to the group's analysis, mean FDG uptake for segments with contrast enhancement of greater than 75% was 60.23 ± 5.02%. For segments with contrast enhancement between 25% and 75%, mean FDG uptake was 72.45 ± 7.57%, and it was 84.19 ± 3.47% for segments with contrast enhancement of less than 25%.
At a cutoff value of 42% transmurality, contrast-enhanced MRI differentiated viable from nonviable heart segments with 71% sensitivity and 71% specificity.
Based on the comparisons, Tian said the study found "some reasonable results for the correlation between contrast-enhanced MRI and FDG-PET, in terms of defining viable and nonviable myocardium. However, these results are from such a small cohort of patients that I think we need a bigger study to see the reproducibility of these results apply to the clinical setting."
Follow-up research
"We are hoping that if we do 30 patients [in a future study] and this data holds up, perhaps we can use this prospectively now to guide therapy in the lab," Dilsizian added.
To a degree, the results are already helping to guide procedures for ventricular tachycardia ablations at the facility.
"In our institute, we are now trying to have the images scanned before the patient undergoes ablation and try to see those images before we go to the electrophysiology lab," Tian said. "We also reconstruct the images into a 3D format and try to provide preprocedural information of the scar location, its size, and where we should allocate more time to map the patient."
She added that the mapping procedure is "very time intensive" and the ablation procedure can take up to eight hours. "So, if we know preprocedurally where the scar is, we can allocate our time better and shorten the procedure."
By Wayne Forrest
AuntMinnie.com staff writer
October 5, 2010
Related Reading
Cardiac MR changes management in 62% of cases, study shows, September 25, 2009
Cardiac MR techniques improve myocardial assessment, June 15, 2009
MRI detects bleeding in the heart after a heart attack, February 13, 2009
MRI can provide safe imaging for pediatric heart patients, August 29, 2008
MRI evaluation of chest pain cuts acute coronary syndrome, August 15, 2008
Copyright © 2010 AuntMinnie.com