A new study has found that FDG-PET/CT can provide important information on patients with Crohn's disease that can help determine whether medical therapy or surgery is the correct course of action.
Not only were FDG-PET/CT images "quite sensitive" to Crohn's disease, but additional analyses using maximum standardized uptake values (SUVs) helped identify patients with active inflammation in the bowel.
Researchers from Johns Hopkins University in Baltimore, Yale University in New Haven, CT, and the University of Toronto in Canada collaborated on the study, published in the November issue of the Journal of Nuclear Medicine (2009, Vol. 50:11, pp. 1751-1759). The lead author is Dr. Heather Jacene in the division of nuclear medicine at Johns Hopkins.
The prospective study analyzed 17 patients with Crohn's disease. The cases included nine woman and eight men, with a median age of 39 years, ranging from 26 to 63 years old. All 17 patients underwent FDG-PET/CT prior to their scheduled surgery for symptoms of bowel obstruction. The patients fasted for at least four hours prior to the scans and intravenous injection of FDG, based on patient height and weight.
PET/CT protocol
After 60-minute FDG uptake, patients received a combined PET/CT scan (Discovery LS, GE Healthcare, Chalfont St. Giles, U.K.) from the midthorax to the pelvis. A noncontrast-enhanced CT scan was obtained first on a four-detector helical scanner.
After the PET/CT scan, eight of the 17 patients received 120 mL of Omnipaque 350 (GE Healthcare) and underwent contrast-enhanced CT. The images once again were taken from the midthorax to the pelvis without the patient leaving the table.
Two readers reviewed the images, looking for FDG uptake in the abdomen or pelvis, which could represent active bowel inflammation. The contrast-enhanced CT scans were used, when necessary, to provide additional information to the PET/CT images to determine the presence or absence of active inflammation or to localize a lesion.
The researchers also sought to determine whether semiquantitative analyses of FDG uptake could measure inflammation. Maximum standardized uptake value corrected for lean body mass (SULmax) was calculated for lesions found by PET/CT that could be active inflammation in the bowel.
Lesion detection
PET/CT detected 33 areas of increased FDG uptake (lesions) in the abdomen, which could represent active inflammation in the bowel. All 17 patients had at least one lesion. The readers concluded with diagnostic certainty that 18 lesions were definitely abnormal and five lesions were probably abnormal. There were equivocal findings for three patients, probably normal lesions in three cases, and definitely normal for four patients.
For the eight patients who received both PET/CT and PET with contrast-enhanced CT, the study ruled that intravenous contrast did not significantly change the conclusion of the PET/CT image, as the same PET findings were seen on both PET/CT and PET with contrast-enhanced CT.
In a semiquantitative PET analysis, researchers determined that cutoff values of 8.0 for SULmax and 223.6 for total inflammation volume (TIV) were the optimal marks to distinguish inflammation and fibrosis or hypertrophy in a patient's bowel.
SULmax results
Based on that calculation, when SULmax was greater than 8, the sensitivity for detecting active inflammation of the bowel was 60%, specificity was 100%, positive predictive value rated 100%, negative predictive value was 78%, and accuracy was 83%.
For TIV greater than 223.6, sensitivity registered 60%, specificity was 71%, positive predictive value was 71%, negative predictive value rated 60%, and accuracy was 67%.
No patient with SULmax less than or equal to 8 had acute inflammation. Two patients presented with acute inflammation and had an SULmax of less than 8. In addition, patients with severe chronic inflammation had significantly higher SULmax than patients with mild or moderate chronic inflammation (8.162.8 versus 4.762.5).
The study also noted that while seven patients had fibrosis or muscle hypertrophy on histology, SULmax was not significantly different among those patients and there was no significant difference in TIV between patients with fibrosis or hypertrophy and inflammation.
 |
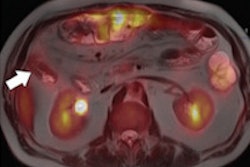
| 33-year-old male with Crohn's disease for three years, presenting with cramps after eating. Small-bowel series and CT scan showed marked thickening of distal ileum with luminal narrowing and proximal dilation of bowel. A PET/CT scan (A and B) revealed intense FDG uptake fusing to thickened ileum (arrows). SULmax was 13, and TIV was 258.2 SUL mL. Intravenous contrast-enhanced CT scan (C) shows mural stratification (arrowhead). In resected terminal ileum (D), there was acute and chronic transmural inflammation (In) and muscularis propria (MP) and muscularis mucosa (MM) hypertrophy and fibrosis. Image courtesy of the Journal of Nuclear Medicine. |
Researchers cited the small study population and the readers' knowledge that the patients had Crohn's disease as two possible limitations of the study. "These factors could have biased the readers to be more sensitive to the detection of any abnormal 18F-FDG uptake in the bowel, which is often variable," they wrote.
While no patients without Crohn's disease were included as a control group, the authors added that the lack of such a group "probably did not alter the results for the specific question being addressed in this study," comparing fibrosis or hypertrophy to inflammation in patients with Crohn's disease and symptoms of bowel obstruction.
The researchers recommend additional studies with a larger patient sample to determine and explore the role of FDG-PET/CT in assessing the efficacy of medical management in treating inflammatory bowel disease.
By Wayne Forrest
AuntMinnie.com staff writer
November 16, 2009
Related Reading
Colonoscopy findings usually not needed for Crohn's treatment decisions, September 28, 2009
Musculoskeletal deficits associated with pediatric Crohn's, January 29, 2009
Crohn's disease patients at risk of significant diagnostic radiation exposure, November 18, 2008
CT enterography answers range of small-bowel questions, May 22, 2007
CT enterography can determine Crohn's disease severity, November 7, 2006
Copyright © 2009 AuntMinnie.com