Image quality was excellent and radiation doses generally low in the first peer-reviewed study of coronary CT angiography (CTA) performed on a 320-slice scanner, which can image the heart in a single beat for most patients.
Researchers from Brigham and Women's Hospital in Boston performed their retrospective peer-reviewed study in 40 consecutive patients who underwent coronary CTA on a 320-detector-row scanner (AquilionONE, Toshiba America Medical Systems, Tustin, CA), a machine that has been installed in only a few sites to date.
"Initial 320-detector-row coronary CT images have consistently excellent quality and iodinated contrast opacification," wrote Dr. Frank Rybicki and his colleagues in the International Journal of Cardiovascular Imaging (March 27, 2008).
Rybicki is an associate professor of radiology at Harvard Medical School in Boston and director of cardiac CT and vascular CT/MRI at Brigham and Women's Hospital. His colleagues include Drs. Hansel Otero, Michael Steigner, Gabriel Vorobiof, Leelakrishna Nallamshetty, and others.
The group cited several theoretical advantages of a 320-detector-row system. AquilionONE features 16 cm of coverage per rotation, compared to 12.8 cm on the 256-slice investigational model that was the system's predecessor. This enables whole-heart coverage, potentially reducing patient radiation by eliminating helical overlap.
Scanning with 320 detector rows also eliminates the stairstep artifact "inherent to 64-slice technology that images subvolumes of the entire cardiac volume over multiple gantry rotations," they wrote.
And 320-slice image acquisition, which can usually cover the heart in a single rotation, theoretically increases opacification while reducing contrast volumes by directing the contrast bolus to a single imaging time point.
 |
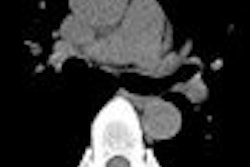
| Volume-rendered image of the heart from 320-detector-row CT scanner of a 45-year-old woman with no evidence of coronary artery disease. AquilionONE CT has no stairstep artifact, as the entire cardiac volume is acquired in a single heartbeat. All images courtesy of Dr. Frank Rybicki. |
The study evaluated 40 consecutive patients (28 men, 12 women; mean age 54; mean BMI 29.1) presenting for the evaluation of chest pain, dyspnea, and/or presurgical evaluation to exclude coronary artery disease.
Axial images were acquired using 320 x 0.5-mm detector configuration, 350-msec gantry rotation, 120 kVp, and either 400 mAs (n = 28) or 580 mAs (n = 12). The decision to use the higher mAs setting depended on body mass index (30 kg/m2 cutoff) and the geometry of the patient's thorax.
"The most common protocol, in 25 of the 40 patients, used prospective gating, a single heartbeat, 120 kVp, 400 mAs, 16 cm of coverage, and a phase window of 60% to 100%," Rybicki told AuntMinnie.com.
To minimize radiation dose, prospective gating was used in 34 patients, and retrospective gating in only the six patients with clinical indication or referrals for functional imaging.
"If the aortic valve or mitral valve is suspected to be abnormal, or if the requesting physician wants a wall motion (analysis) or ejection fraction, we do retrospective gating; otherwise, we do prospective gating," Rybicki said.
Before the scans, all patients received 80 mL of 370 mg I/mL iopamidol (Isovue 370, Bracco Diagnostics, Princeton, NJ) iodinated contrast, followed by 40 mL of saline administered at 6 mL/sec (Empower CTA dual injector, E-Z-EM, Lake Success, NY). All patients received 0.4 mg of sublingual nitroglycerin before imaging, and those with resting heart rates greater than 65 bpm received intravenous metropolol beta-blockage in 5-mg increments. The mean heart rate at CT imaging was 61 (range 45-82) bpm.
The image data were reconstructed at 0.5-mm intervals and evaluated on a Vitrea 4.0 workstation (Vital Images, Minnetonka, MN) by two experienced readers who applied the American Heart Association's 15-segment model. They rated the images subjectively for quality on a scale of 1 to 4, with 4 being excellent and 1 nonevaluable.
In all, 34 patients were scanned during a single heartbeat, most commonly using a phase window of 60% to 100%. Six patients whose heartbeats could not be lowered to 65 bpm with beta-blockers were scanned over two heartbeats, Rybicki said.
The group also estimated effective radiation doses for prospective versus retrospective ECG gating, two body mass index categories, and acquisition in one versus two heartbeats.
According to the results, more than 89% of the segments were rated excellent (reader 1 89.9%, 517/583; reader 2 88.7%, 524/583) following elimination of 17 segments that were too small to be characterized (< 1.5 mm), were occluded, or were not present in the patient's anatomy. All but one of the remaining segments was rated 2 or 3.
The researchers documented the cause of image degradation for every segment not rated excellent, with cardiac motion cited most frequently.
Combining the scores from both readers, 82 segments had motion artifact, "but we were able to read through the motion because it was not severe," Rybicki said. A total of 36 of 593 segments were limited by image noise, with significantly more of these segments (p < 0.001) imaged at 580 mAs. The average BMI of patients with segments limited by noise was 37.8, Rybicki said. Five additional segments had significant beam-hardening artifact.
 |
| Multiplanar reformatted coronary CT image (left) from 320-detector-row CT shows a midright coronary artery aneurysm (arrow) confirmed by coronary catheterization (right). The CT image was acquired in a 60-year-old man using 320-slice CT in a single heartbeat using 80 cc of iodinated contrast. Prospective ECG gating was used, and patient radiation dose was approximately 5 mSv. |
Contrast opacification as measured by Hounsfield units was almost universally excellent, at a mean of 350 HU overall, and a contrast opacification gradient of 30-50 HU, the authors wrote. The mean radiation dose was 6.8 ± 1.4 mSv.
For this study the patients were scanned with conservative protocols, as befitting a new technology, with regard to iodine load, the prospective ECG-gating phase window, and craniocaudal coverage, the researchers wrote.
Image quality was enhanced by the large contrast volume, aggressive beta-blockade, and a relatively wide phase window that enabled additional reconstructions for patients with subtle motion artifact.
Future work will focus on lowering dose and contrast volume while maintaining high image quality, they added.
Some believe the conservative phase window of 60% to 100% used in the study is wider than necessary for prospectively gated exams, Rybicki said. Using a narrower window does reduce the radiation dose.
"If you were to lower the phase window from 40% to 10% and decrease the craniocaudal coverage to 14 mm instead of 16 mm, you could reduce the mean dose to 4.0 mSv," he said. "We've done it, but not in this paper."
The highest dose for prospective gating was 9.4 mSv and 18.1 mSv for retrospective gating. The mean dose for retrospectively gated exams was 14.0 mSv, the authors reported.
Overall the 320-detector-row coronary CT images had consistently excellent quality and opacification, the authors concluded.
"You get an extraordinarily high number of evaluable segments in a single heartbeat, and there are no stairstep artifacts. That's the real advantage of this scanner," Rybicki said. "Because you image the heart in one beat, you can study the way the contrast enters the coronary arteries and myocardium, so you can study the differences in contrast opacification across lesions and in the myocardium."
In that vein, a study the authors are preparing to submit for the 2008 RSNA meeting in Chicago will analyze how contrast density corresponds with the percentage of stenosis and other lesion characteristics, he said.
By Eric Barnes
AuntMinnie.com staff writer
April 7, 2008
Related Reading
Prospective gating drops cardiac CT radiation dose, March 10, 2008
New studies examine CR, CT radiation dose, March 9, 2008
Toshiba basks in AquilionONE glow, but more work remains, December 24, 2007
AquilionONE 320-slice CT scanner spearheads Toshiba RSNA launches, November 26, 2007
256-slice perfusion CT equivalent to SPECT for arteriosclerosis detection, November 13, 2007
Copyright © 2008 AuntMinnie.com