U.S. researchers will use this week's European Congress of Radiology in Vienna to present research that shows dual-source CT (DSCT) making inroads into cardiac functional imaging, an area currently dominated by SPECT. The study moves dual-source coronary CT angiography (CTA) closer to the holy grail of cardiac imaging -- a test that performs both morphological and functional analysis in a single scan.
Researchers from the Medical University of South Carolina (MUSC) at Charleston believe that dual-source CT has a bright future in assessing myocardial blood pool in addition to the coronary artery morphology, lending insight to the significance of stenotic lesions on cardiac function.
"One of the major benefits for the patients is that in a single scan we can actually do (coronary artery) plaque characterization, and also myocardial blood-pool scanning," said principal investigator Dr. Balázs Ruzsics, Ph.D., from MUSC's radiology department, in an interview with AuntMinnie.com.
The results will be presented as presentation B-556 on Sunday, March 9, in the ECR session SS 1003, "Myocardial and pericardial diseases," from 10:30 a.m. to 12:00 p.m. in room R2.
A one-stop shop?
According to the researchers, DSCT can provide information about relevant coronary artery stenoses and also assess whether the lesions are causing a strain on the heart, leaving patients vulnerable to a heart attack.
"One guy might have strong collateralization -- enough blood coming from other vessels -- that a stenosis doesn't mean anything for that person," said co-investigator Dr. U. Joseph Schoepf, an associate professor of radiology at MUSC. "Other people have less well-organized collaterals, and they get chest pain or even myocardial infarction from such a lesion."
The need to evaluate the significance of stenotic lesions on heart function is why two exams are generally needed to perform a complete cardiac workup. While stenosis can be evaluated with conventional coronary angiography or coronary CTA, a functional test such as a nuclear stress test is needed to assess lesion severity, Schoepf said.
"You can also replace nuclear medicine with MR," he added. "Or the simplest way is to put the patient on a treadmill and find out if the (ECG) shows ischemia."
The use of dual-source CTA as a functional test exploits the fact that human tissues reveal different absorption characteristics when penetrated with different x-ray energy spectra. The researchers created iodine maps based on this difference to analyze the myocardial blood pool.
Depending on the energy setting for each x-ray tube, "iodine has very different absorption characteristics in the myocardium," Schoepf said. "So we can map areas in the heart muscle that have no iodine, ergo, no blood. The latter is only made possible by the dual-source application."
For the study, the researchers used a dual-source CT scanner (Somatom Definition, Siemens Medical Solutions, Malvern, PA), which has two x-ray tubes and two detector arrays mounted in a single gantry. In dual-energy mode, the x-ray tubes are set to different output levels.
 |
 |
| In a 64-year-old man presenting with chest pain, 3D and multiplanar reconstructions of coronary CTA images show a significant stenosis in the first diagonal branch of the left anterior descending (LAD) artery and a 70% stenosis in the mid right circumflex artery (RCA) (arrows). All images courtesy of Dr. Balázs Ruzsics, Ph.D., and Dr. U. Joseph Schoepf. |
 |
 |
One x-ray tube was operated at 150 mAs per rotation at 140 kV, with the second tube set at 165 mAs and 100 kV or 80 kV, depending on body habitus, the group explained in a study abstract.
They examined 35 patients (25 men, 10 women; average age 63 ± 11 years) presenting to the emergency department with chest pain, all of whom were referred for the evaluation of suspected coronary artery disease (CAD).
The patients underwent contrast-enhanced retrospectively ECG-gated DSCT coronary angiography with ECG signals acquired simultaneously. Settings included 64 x 0.6-mm collimation using a z-flying focal spot technique, 330-msec rotation speed, pitch of 0.2, mAs of 165, and kVp of 80-100 depending on body habitus. The scan delay was determined by test bolus injection of a nonionic contrast agent at 6 mL/sec. From each scan, three reconstructions were made using 0.75-mm section widths and 0.4-mm reconstruction increments.
Sixteen of the 35 patients in the study had undergone rest and stress nuclear perfusion imaging using SPECT, while another 13 had undergone conventional angiography, and five had all three tests, according to the researchers. Two readers working independently evaluated each coronary artery segment in each available test, comparing the results in the available modalities for each patient.
Image analysis was performed by mapping the distribution of myocardial iodine distribution from the low kVp spectra on virtual noncontrast multiplanar reformats of the myocardium in long- and short-axis views, the group noted in the abstract. Two observers independently analyzed all dual-source CTA studies for myocardial blood-pool deficits using the American Heart Association's 17-segment model.
 |
| In a 64-year-old man with chest pain, conventional catheter angiography confirmed the coronary CTA findings, and described a 50% ostial stenosis with diffuse disease throughout the vessel and a discrete 90% stenosis in the mid right circumflex artery (RCA) (arrows). |
 |
"Segmental comparison was performed between coronary CTA and (DSCT) myocardial segments," they wrote. "Results were also compared with findings at SPECT and/or invasive catheter angiography. Data were analyzed using the Bayesian model."
The coronary CTA results revealed significant coronary artery stenosis (> 50%) in 16 of the 35 patients. Compared to conventional catheter-based angiography, coronary CTA had sensitivity of 98%, specificity of 88%, and accuracy of 92% for detecting coronary artery stenosis.
SPECT revealed fixed myocardial ischemia in five patients and reversible myocardial ischemia in 11 patients. Dual-source CTA blood-pool imaging correctly identified 90% of the fixed and 88% of the reversible myocardial perfusion deficits seen at SPECT, Schoepf and Ruzsics said.
Compared to SPECT, dual-source CT had 91% sensitivity, 91% specificity, and 91% accuracy for detecting myocardial ischemia by segment, Schoepf said. Compared to coronary catheterization, dual-source CTA had 92% sensitivity, 79% specificity, and 90% accuracy for detecting myocardial ischemia by segment.
 |
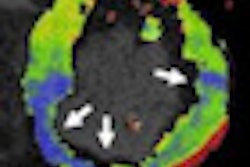
| In a 64-year-old man with chest pain, colored regions of blood-pool images represent iodine, while the darker parts of the myocardium depict ischemia as a lack of contrast uptake. Arrows indicate the myocardial blood-pool deficit, i.e., ischemia. |
 |
 |
For blood-pool imaging, it's more relevant to compare dual-source CT to SPECT, rather than conventional angiography, Schoepf noted. "We just threw in coronary angiography because we didn't have SPECT correlation in all patients," he said. Coronary angiography isn't the best tool for producing blood-pool maps because it shows only stenoses, which may not be hemodynamically significant, he added. The exams have been performed, but not yet analyzed, in an additional 15 patients.
In all territories where dual-source CTA showed blood-pool deficits, SPECT or catheter angiography confirmed ischemia or critical stenosis, they concluded.
Radiation doses for the retrospectively gated coronary CTA scans ranged from approximately 7 mSv to 15 mSv per patient, depending on gender and patient habitus, the researchers told AuntMinnie.com.
Ultralow-dose prospectively gated coronary CTA (typically delivering from 2 mSv to 5 mSv) isn't feasible for functional imaging. However, eliminating the need for SPECT (7 mSv to 25 mSv) in this group of patients more than compensates for the higher dose delivered in z-axis-modulated, retrospectively gated dual-source CTA compared to prospectively gated coronary CTA, Schoepf said.
 |
| In a 64-year-old man with chest pain, image of the corresponding slice shows inferior ischemia (arrows). |
The MUSC group does not typically use beta-blockers in dual-source CT cardiac imaging, primarily due to logistical difficulties created by the need to wait for the drugs to take effect. Beta-blockers were not used in the present study, but Schoepf said the group "struck it lucky" with its cohort, which had a low mean heart rate of 57 ± 9 bpm.
Clinicians need to look at the stenosis, as well as its physiological and hemodynamic consequences, to determine the best course of patient management, according to Schoepf. "The beauty of blood-pool imaging with the dual-energy approach is that it brings it together in a single scan," he said.
"One of the major benefits for the patient is that in a single scan (you) can actually ... do plaque characterization and also myocardial blood-pool scanning," Ruzsics added. "We can also nail down whether any of that plaque can cause a significant stenosis -- i.e., a blood-pool defect in the myocardium."
Dual-source coronary CTA could also be used to perform delayed-enhancement imaging for assessing myocardial viability, according to Schoepf.
"I don't like the term 'one-stop shop,' but with this we're getting close," Schoepf added.
By Eric Barnes
AuntMinnie.com staff writer
March 6, 2008
Related Reading
DSCT matches angiography for stenosis detection -- even in fast hearts, December 4, 2007
Michigan heart center aims DSCT guns at image quality, October 8, 2007
CTA predicts functional recovery of the myocardium, September 7, 2007
Dual-source coronary CTA images the calcium-burdened, April 13, 2007
Dual-source imaging promises better CT scanning, June 15, 2007
Copyright © 2008 AuntMinnie.com