CHICAGO - When performing MR angiography, functional MRI, and MR cholangiopancreatography procedures on pediatric patients, a 3-tesla magnet is the preferred modality at the Hospital for Sick Children of the University of Toronto. Three-tesla MRI offers good signal-to-noise ratio and image quality, faster imaging capability, improved resolution visualizing small vessels and ducts, and improved spectral resolution in spectroscopy compared to 1.5-tesla MRI.
Three-tesla MRI also offers the advantage of being able to acquire thin-slice, high-resolution images in a shorter overall exam time compared to 1.5-tesla MRI. This is especially beneficial when imaging infants and very small children.
After performing more than 2,500 3-tesla MRI exams of children ages 7 days to 18 years in a 12-month period, radiologists affiliated with the Canadian children's hospital candidly describe the challenges and experiences they encountered in a poster presented at the 2008 RSNA annual meeting.
At the time the 3-tesla MRI was installed at the Hospital for Sick Children, few peer-review journal articles had been published about the use of 3-tesla MRI with pediatric patients, especially with respect to clinical experiences. The radiologists and technologists faced the challenges of unfamiliarity with using the system, safety concerns, and artifacts degrading imaging quality. The diagnostic imaging department took an approach of "one problem at a time," according to lead author Dr. Govind Chavhan.
Initial implementation and safety precautions
The first initiative was to develop protocols to reduce artifacts and obtain image quality comparable to the level of 1.5-tesla MRI. The 3-tesla MRI (Achieva, Philips Healthcare, Andover, MA) was first used for neurology imaging, and for the first three months the system was not used with children who had recently undergone surgery or received implants. Other procedures were added gradually, and restrictions against imaging children with Bioclips (Bioplate, Los Angeles), port-a-cath devices, and braces were lifted.
For safety reasons, the department required that physicians ordering an MRI procedure complete the screening form with precision and accuracy to avoid any accidents, Chavhan reported. Heat and acoustic noise were also of concern. The body temperature of patients was monitored for an initial six-month period. During this period of time, no signs of body heating associated with 3-tesla MRI imaging were detected, so this was discontinued. However, all patients are required to have normal blood pressure, oxygen saturation, and other vital signs confirmed immediately prior to a procedure.
The acoustic noise of a 3-tesla magnet is louder than a 1.5-tesla magnet, and this has been an issue because some children are sensitive to the noise and find it disturbing. All children wear headphones and earplugs, as does anyone who stays in the suite with the patient. Patients may wear movie goggles as well.
To prevent patients from becoming dizzy or nauseous, technologists were instructed to move the modality table very slowly when placing patients inside the bore. Exams are rescheduled if a patient feels nauseous, dizzy, or lightheaded. One parent is allowed to be with the patient in the MRI suite, but he or she is required to sit in a chair positioned a minimum of 7 ft from the bore.
To avoid inducing magnetic field and potential burns, patients are never positioned with crossed arms or legs. If their bodies ever feel hot, the technologists halt the procedure until they have consulted with a radiologist. All exams are performed within a 60-minute time frame. Technologists communicate with the patient and any adult in the MRI suite after every sequence.
Artifacts
Flow artifacts in the spine and posterior cranial fossa, as well as dielectric, graininess in the center of the field-of-view, susceptibility, and chemical shift-related artifacts, are commonly seen. Use of saturation bands and flow compensation can reduce flow artifacts in posterior cranial fossa seen mainly on T2-weighted images.
Dielectric effects are caused by shorter wavelength (27 cm), resulting in field focusing and more pronounced energy disposition in deep central parts of body. Dielectric effect-related artifacts are seen as areas of altered signal and can be reduced by placing high-definition content, such as ultrasound gel, on the anterior abdominal wall. The appearance of defects can also be reduced by using image correction software.
The authors speculate that graininess, which they most often see in the center of the field-of-view, is related to the system's coils, as this area is the farthest away from the coils. Local shimming and frequency offset tests are available for use on the MRI system to reduce susceptibility artifacts. They report that a frequency offset test can be performed quickly to determine the optimal fat saturation offset in Hz. This exact value is then put in the sequence parameter to optimize fat suppression.
Challenges with sequences
T1-weighted turbo spin-echo (TSE) sequences at 3-tesla are longer, limited by a specific absorption ratio. They are prone to artifacts, and contrast on T1-weighted TSE sequences between tissues was also poor. Use of the fluid-attenuated inversion recovery (FLAIR) T1-weighted TSE sequence in the brain improves gray-white contrast, the radiologists discovered. They tended to use T1 with gradient echo, such as T1-weighted turbo field-echo (TFE), as an option for providing reasonable quality T1-weighted images. T1-weighted 3D TFE sequences proved better, providing excellent quality images in the brain, as well as in the spine.
T2-weighted fast spin-echo (FSE) images in the chest, abdomen, and spine are affected by flow and motion artifacts, but the authors noted that if flow-related issues and inhomogeneity are resolved, T2-weighted FSE gives excellent quality images. Single-shot FSE sequences with long echo train length are affected by reducing T2 and B1 inhomogeneity on 3-tesla. However, reducing echo train length by using parallel imaging also works well.
The reduced imaging time improves image quality in uncooperative children. Because of inherent high signal-to-noise signal intensity of static fluid components, the quality of MR cholangiopancreatography (MRCP), myelography, and noncontrast urography was excellent. However, balanced TFE sequences are affected by susceptibility artifacts, and the quality of a 3-tesla image is not significantly different from that of 1.5-tesla images, according to Chavhan and colleagues.
Body imaging
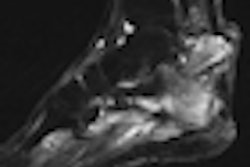
Musculoskeletal imaging has proved to be an excellent application for 3-tesla MRI imaging. Superior image quality with better visualization of cartilage and ligaments was seen in all of the 188 body imaging procedures that the hospital has performed to date. The authors attribute superior image quality to reduced scan times, the ability to acquire thin sections, and high spatial resolution for small field-of-view images, all of which help offset body motion and tissue inhomogeneity that produce artifacts. They found it useful to perform single shot sequences to obtain artifact-free images of chest and abdomen parallel imaging.
In the year that the 3-tesla magnet has been used, more than 15 MRCP examinations of diagnostic quality have been performed to evaluate the biliary and pancreatic ductal systems of pediatric patients. There is also improved visualization of small peripheral intrahepatic ducts and the pancreatic duct using 3-tesla instead of 1.5-tesla. Superior anatomic details were also seen in imaging perianal fistulas in pediatric patients with Crohn's disease, but the authors reported comparable quality for whole-body MRI scans.
Head imaging and MR angiography
A total of 1,506 brain examinations have been performed in the first year of use. The quality of exams of MR angiography, BOLD-function MRI, epilepsy imaging, and inner ear imaging have significantly improved with use of 3-tesla MRI compared to 1.5-tesla MRI.
MR angiography is consistently superior. Visualization of small vessels was significantly better in terms of number and size, the authors reported. Thin sections and high spatial resolution of 3-tesla MRI provided superior anatomic details. They discovered that prominent perivascular spaces are routinely observed and that globus pallidus is often hypointense on T2 images due to susceptibility effects.
Hippocampal anatomy and cortical dysplasias were better visualized, as well as visualization of small nerves and vessels in the posterior fossa with increased clarity of cisternal nerve roots. All of these factors have made 3-tesla MRI the preferred system for epilepsy imaging, inner ear imaging, posterior fossa imaging, and MR angiography.
Research determined that it is also possible to use half the dose of gadolinium as would be used with a 1.5-tesla MRI system, and yet achieve the same degree of contrast enhancement. The radiologists at the Hospital for Sick Children have not yet attempted gadolinium dose reduction, but they found that in general, contrast enhancement is better than when using a 1.5-tesla MRI. Single voxel spectroscopy is routinely performed, with much improved spectral separation.
"Spine imaging is still a troubled territory on 3-tesla in our experience," the authors noted, which included 362 examinations. "Most of our spine studies are performed for evaluation of thecal sac and cord pathologies. In our experience, conspicuity of the cord is reduced on T2-weighted images that are significantly affected by flow artifacts. Cord conspicuity is also reduced on T1-weighted images from prolonged T1-relaxivity."
Chavhan and colleagues noted that they were still in the process of learning and improving techniques, and the effects of this on the diagnostic ability and clinical utility of a 3-tesla MRI are still not fully defined. They feel that a second year of utilization may increase throughput in the 3-tesla MRI suite, especially regarding musculoskeletal imaging.
By Cynthia Keen
AuntMinnie.com staff writer
December 2, 2008
Related Reading
3-tesla MRI superior to 1.5-tesla MRI in epilepsy evaluation, October 1, 2008
MRI's clinical role expands with new expectations, March 1, 2007
Copyright © 2008 AuntMinnie.com