Small developmental venous anomalies (DVAs) can be overlooked, even with contrast-enhanced MRI exams, if the images are not examined carefully, but DVAs that have collecting veins with larger diameters are more visible, according to a new study in Clinical Neuroradiology (November 17, 2013).
DVAs are the most frequently encountered cerebral vascular malformations, with an incidence of 2.6% from previous research, the study authors noted. Although most DVAs are discovered incidentally and show no clinical significance, the diagnosis of a DVA has often generated concern among many physicians who are less familiar with the field of intracranial vascular malformations.
To clarify the clinical question, researchers from Gaziosmanpaşa University in Turkey decided to evaluate the morphological features of DVAs based on MRI findings. The team found that radiologists are sometimes unable to recognize DVAs, according to lead author Dr. Erkan Gökçe, an assistant professor in the department of radiology.
A unique aspect of this study is that, unlike in other previous research, the team studied the diameter of the DVA collector vein, as well as the relationship between its visibility and MRI examinations, he explained.
Gökçe and colleagues performed a retrospective analysis of contrast-enhanced cranial MRI exams of 1,165 patients seen for various reasons. The study participants' age ranged from 4 to 84. The imaging had been conducted from September 2009 to January 2013.
The images were examined for DVA location, the number of collecting veins, collecting vein diameter, drainage veins and sinuses, any accompanying parenchymal abnormalities or lesions, and the visibility of the DVA on MRI.
The study included 75 patients diagnosed with DVAs: 45 were female and 30 were male. The researchers performed 3D spoiled gradient-echo (SPGR) sequences in 57 patients, spin-echo T1-weighted sequences in 10 patients, and both 3D SPGR and spin-echo T1-weighted contrast-enhanced brain MRI examinations in eight patients.
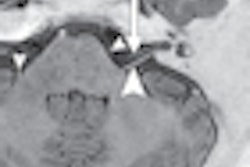
The researchers defined DVAs as vascular structures that passed cerebral or cerebellar parenchyma in different lengths and that were characterized by the clustering of venous stems uniting in a collecting vein that causes the typical "Medusa head" appearance. Image findings were diagnosed as DVA with consensus after being evaluated by two radiologists.
Here are some of the key results:
- A total of 88 DVAs were observed.
- The frequency of DVAs found on contrast-enhanced cranial MRI was 6.4%, which was higher than the frequency determined in the literature.
- Single DVAs were observed in 65 patients, two were seen in seven patients, and three were observed in three patients.
- Sixty-four (72.7%) of the DVAs were located in the supratentorial region, and 24 (27.3%) were located in the infratentorial region. Forty-eight (54.5%) of the DVAs were located in the right cerebellar or cerebral hemisphere, while 37 (42.0%) were in the left cerebellar or cerebral hemisphere, one (1.1%) was in both cerebellar hemispheres, and two (2.3%) were found in the midline of the pons.
- Collecting vein diameters ranged from a minimum of 1.0 mm to a maximum of 4.3 mm (median 2.0 mm).
- In DVAs that had multiple collecting veins, the collecting vein diameters ranged between 1.2 mm and 4.3 mm (mean 2.39 ± 0.91 mm).
- A total of 98 collecting veins were identified, with a single vein identified in 80 DVAs.
- A statistically significant difference was found in the diameter of the collecting veins between DVAs that were visible and nonvisible on noncontrast MRI.
The authors noted that in their research nearly half of the DVAs (45.5%) could not be visualized on routine noncontrast MRI exams, as they found a statistically significant difference between the visibility of DVAs and the collecting vein diameter.
DVAs with an average 2.3-mm collecting vein diameter could be observed in an unenhanced series, and DVAs with an average 1.7-mm diameter were not visible. That is why it is necessary to perform contrast-enhanced cranial MRI exams to visualize DVAs, they explained.
However, they cautioned that small DVAs that have a collecting vein of small diameters can be overlooked, even in a contrast-enhanced series if it is not analyzed carefully.
Parenchymal abnormalities or lesions accompanying a DVA did not improve visibility on noncontrast imaging, and the visibility of the DVAs accompanied by a cavernoma in a noncontrast series also was not statistically significant.
The authors recommended that contrast-enhanced MRI should be conducted to visualize accompanying DVAs in patients diagnosed with cavernoma because of the frequency of the association between DVA and cavernoma.