Which modality should be used to guide brachytherapy treatments, MRI or CT? Both have strengths and weaknesses, but either is superior to traditional 2D x-ray guidance, which is still used in nearly half of U.S. cancer treatment centers.
That's the conclusion of a debate on the relative merits of MRI and CT brachytherapy guidance that took place at the American Brachytherapy Society (ABS) meeting in San Diego in April. Taking sides were Dr. Sudershan Bhatia, PhD, of the University of Iowa radiation oncology department, and Dr. Catheryn Yashar, of the radiation oncology department at the University of California, San Diego (UCSD).
Better than x-ray
Both radiation oncologists agreed that MRI and CT are superior to the 2D approach of x-ray, which is still used by an estimated 43% of U.S. cancer treatment centers.
"We are moving from imagination-guided brachytherapy to image-guided brachytherapy," Bhatia said.
But, Yashar pointed out, CT works very well at half the cost of MR -- and without moving a patient full of instruments around to get to the magnet. Treatment should be affordable, workable, and effective, which CT provides.
Access to quality 3D imaging, particularly during procedures, remains a challenge for many centers. MRI was declared the gold standard for designing brachytherapy treatment for cervical cancer in 2005 by a working group of the Groupe Européen de Curiethérapie and European Society for Therapeutic Radiology and Oncology (GEC-ESTRO), but the vast majority of radiation oncologists are lucky if they have an initial MRI scan from which to work.
An informal survey of the audience at the ABS debate found that less than half have access to an MRI scanner. Those results, Bhatia said, are similar to a study of imaging in Canadian radiation oncology centers in 2010 as part of the International Study on MRI-Guided Brachytherapy in Locally Advanced Cervical Cancer (EMBRACE).
The Canadians found that 50% of centers were still using x-ray, 45% were using CT, and 5% have access to an MRI scanner. Of the centers still using x-ray, 73% planned to go to 3D imaging, with the majority planning to purchase CT systems. Eighty percent of respondents agreed that 3D imaging for brachytherapy should become the standard of care for treating cervical cancer in Canada.
A 2005 review of 36 British cancer centers found even fewer using advanced 3D imaging.
About 10% of the practitioners at the ABS conference reported that they could image and treat in the same room, similar to the outcome of larger and more formal polls. Most obtain imaging studies well in advance.
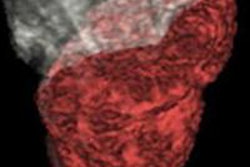
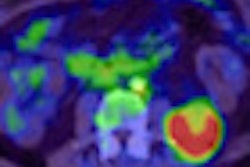
Yashar and Bhatia presented side-by-side CT and MR images of the same anonymized patients, with consistently more definition in the MRI study.
"With the MRI, you have more information," Bhatia said. "CT does not show bulky tumors as distinctly. It's only MR that can show you all the details."
Not only does MRI better stage cervical cancer, it better depicts the soft tissue and enables the reader to discriminate between the tumor and the structures around it in real-time, not created by reconstruction, Bhatia said.
CT is adequate for planning, but its drawbacks must be understood, according to Yashar. For example, CT overestimates the size of the tumor, especially the width, she said, citing a 2005 study.
MRI not perfect?
But MRI has its problems, too.
MRI can also distort, there can be displacement, and there are problems with applicators. "Vitamin E catheter works best," Bhatia noted.
The biggest problems with MRI are the cost and access issues, Yashar said, noting that MRI studies cost nearly 10 times what CT studies cost at UCSD.
"For early disease, I'm not sure MRI gives me data I really have to have," she said. "You don't need an MRI to tell you if there's gross disease outside the cervix."
Yashar conceded that having access to an MRI scanner is ideal. But is it crucial in every patient at every fraction?
"I'm not saying that an MRI isn't helpful," she said. "I'm saying that an MRI isn't going to make the critical decisions -- you have to make that decision. An MRI and CT are not substitutes for being a good physician."
The core question, according to Dr. Anuj Peddada, a radiation oncologist with Memorial Health System in Colorado who moderated the talk, was simple: "Have we improved the cure rates from any of these advanced technologies?"