Researchers at Memorial Sloan-Kettering Cancer Center in New York City say MRI is useful in determining the anatomic origin of uterine cancer and also provides helpful information regarding invasion of adjacent structures, according to a study published online January 6 in Radiology.
The study's authors, led by Hebert Alberto Vargas, MD, noted that MRI's ability to determine the origin of uterine cancer -- whether it's the corpus or cervix -- is critical to appropriate treatment planning.
"Most corpus carcinomas are simultaneously staged and treated with surgery (hysterectomy and bilateral salpingo-oophorectomy)," Vargas and colleagues wrote, "while generally only early-stage cervical cancers are treated with surgery, and advanced cervical disease is treated with chemotherapy and radiation therapy."
A search of Sloan-Kettering hospital records from January 2000 to December 2009 found that 59 patients met the inclusion criterion of having received pretreatment pelvic MR imaging due to uncertainty about the site of newly diagnosed uterine cancer. The patients had a median age of 59 years (range, 28 to 84).
All patients were imaged on a 1.5-tesla MRI system (Signa, GE Healthcare, Chalfont St. Giles, U.K.) with a body coil and a pelvic phased-array coil.
Of the 59 patients, 48 underwent treatment with hysterectomy within six months after MRI and received no other form of treatment between the MRI scan and the hysterectomy. Eleven patients did not receive surgery due to an advanced stage of disease, lack of indication, presence of contraindications for surgery, or patient choice.
In the patients who underwent hysterectomy, the median time between MRI and surgery was 13 days, ranging from 0 to 179 days.
Two readers independently evaluated all MR images by ranking the probability of the anatomic site of the uterine cancer for each patient on a five-point scale: A score of 1 indicated definitive corpus cancer, 2 was probable corpus cancer, 3 was indeterminate, 4 was probable cervical cancer, and 5 was definitive cervical cancer.
If a tumor extended across the corpus and cervix or if more than one tumor was present, the site of origin was assessed subjectively by establishing the location where the tumor appeared to be centered and in which region most of it was situated.
 |
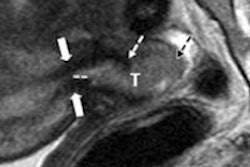
| MR image of an 83-year-old woman shows a large tumor (T) of intermediate signal intensity expanding the endometrial cavity. Pathologic diagnosis from the hysterectomy specimen was a clear cell carcinoma arising from the corpus. All images courtesy of Radiology. |
Of the 48 patients who had surgery for the treatment of uterine cancer within six months of MR imaging, 32 had uterine corpus cancer and 16 had uterine cervical cancer.
"When a reader attributed a tumor's origin to either the uterine corpus or cervix, the odds of the tumor originating from that site were 4.80-6.35 times greater than they would have been if no other information were available," Vargas and colleagues wrote.
They also noted that accuracy levels in detecting cancer invasion of the myometrium, cervical stroma, parametria and/or adnexae, and vagina, respectively, were 72%, 69%, 74%, and 85% for reader 1 and 78%, 77%, 76%, and 85% for reader 2.
 |
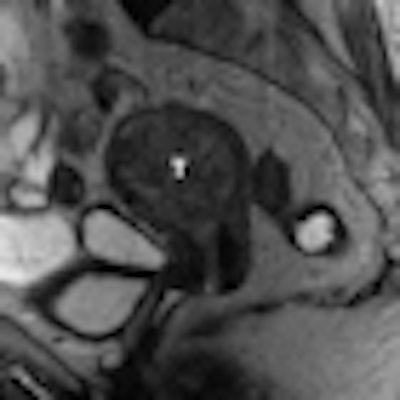
| MR image of a 67-year-old woman shows tumors (T) of intermediate signal intensity in both the endometrial cavity and cervix. The primary origin could not be determined from the MRI scan. Final pathologic diagnosis from the hysterectomy specimen was papillary serous carcinoma of the endometrium with deep myometrial and cervical stromal involvement. |
Of the 11 patients who did not have surgery, seven were thought to have advanced cervical cancer based on clinical examination and imaging and underwent radiation therapy and/or chemotherapy. Both readers were able to identify the origin site as the cervix, as well as advanced disease features, in all seven patients.
The authors cited several limitations of the study, including the retrospective nature of the analysis over a 10-year period.
"Potential changes in the clinical, pathology, and imaging fields and the effect of these changes on our findings were not taken into account," they wrote. "Although the changes that occurred in MR imaging parameters over the course of the 10-year period as a result of the natural evolution of MR imaging technique were not substantial, their effect on the readers' performance remains unknown."
They also noted that while the median time between MRI and surgery was 13 days, a delay of as long as six months may have influenced the results.
However, based on the findings, Vargas and colleagues concluded that MRI can help determine the origin of uterine cancer when clinical and histologic findings are indeterminate. In addition, MRI "may provide information regarding the extent of the disease and invasion of adjacent structures that has important prognostic and treatment planning implications," they wrote.
By Wayne Forrest
AuntMinnie.com staff writer
January 26, 2011
Related Reading
MRI aids US in detecting placenta accreta in pregnant women, January 6, 2010
MRI improves diagnosis of severe endometriosis, July 8, 2009
Study: MRI identifies submucosal fibroids that may migrate into endometrium, May 19, 2008
Some women at long-term cervical cancer risk, October 26, 2007
3-tesla MRI sheds light on shading sign in endometriosis, June 8, 2007
Copyright © 2011 AuntMinnie.com