

Kinetic curves of malignant breast lesions are not consistent across MRI systems, which could potentially lead to clinical problems, according to a study published in the September issue of the American Journal of Roentgenology.
Researchers at the University of Chicago in Illinois compared MRI kinetic curve data gathered by three systems in evaluating malignant lesions of the breast. Based on the study results, Dr. Sanaz Jansen and colleagues concluded that there's a need for improved standardization of breast dynamic contrast-enhanced MRI acquisition (AJR, September 2009, Vol. 193:2, pp. 832-839).
Jansen's team reviewed the cases of 601 patients with 682 breast lesions, 185 benign and 497 malignant, keeping in mind two general principles: malignant lesions show rapid uptake and washout, while benign lesions have slower uptake and persistent contrast uptake over time; and the kinetic characteristics of ductal carcinoma in situ are variable, overlapping with those of benign lesions and showing slower contrast uptake and washout than invasive ductal carcinoma.
"Standardization of breast MRI acquisition is not widespread," the authors wrote. "There are no universally applied quality assurance procedures to ensure that as newer MRI systems are used clinically, the measured kinetic curves continue to satisfy these two general principles."
Malignant lesions were classified as ductal carcinoma in situ, invasive ductal carcinoma, and other. The dynamic MRI protocol consisted of one unenhanced and three to seven contrast-enhanced images taken with one of three imaging protocols and systems:
- System 1: 1.5-tesla Genesis Signa (GE Healthcare, Chalfont St. Giles, U.K.)
- System 2: 1.5-tesla Signa Excite (GE Healthcare)
- System 3: 1.5-tesla Achieva (Philips Healthcare, Andover, MA)
System 1 imaged 137 benign and 304 malignant lesions, system 2 imaged 21 benign and 107 malignant lesions, and system 3 imaged 27 benign and 86 malignant lesions.
 |
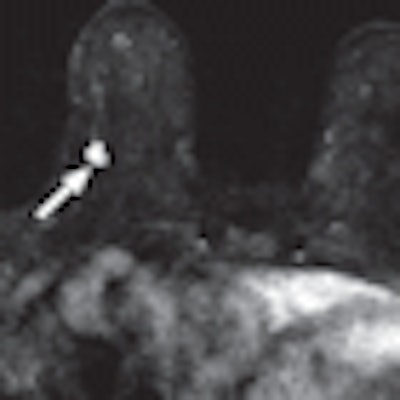
| Examples of MR images and kinetic curves obtained with three systems and protocols. A and B, 57-year-old woman with invasive ductal carcinoma (arrow). MR image (A) and kinetic curve (B) acquired with imaging protocol and system 1 have the following quantitative parameters: initial enhancement percentage, 334%; peak enhancement percentage, 350%; signal enhancement ratio, 1.21; time to peak enhancement, 249 seconds. All images courtesy of the American College of Radiology. |
 |
| C and D, 54-year-old woman with invasive ductal carcinoma (arrow). MR image (C) and kinetic curve (D) acquired with imaging protocol and system 2 have the following quantitative parameters: initial enhancement percentage, 282%; peak enhancement percentage, 360%; signal enhancement ratio, 0.92; time to peak enhancement, 118 seconds. |
 |
| E and F, 73-year-old woman with invasive ductal carcinoma (arrow). MR image (E) and kinetic curve (F) acquired with imaging protocol and system 3 have the following quantitative parameters: initial enhancement percentage, 107%; peak enhancement percentage, 221%; signal enhancement ratio, 0.55; time to peak enhancement, 120 seconds. |
Kinetic curves of malignant lesions imaged with protocol and system 1 showed a higher proportion (89%) of curves with a rapid initial rise, compared with 55% of benign lesions. Malignant lesions imaged with systems 2 and 3 showed comparable proportions of rapid curves compared with their benign counterparts. For all three protocols, more malignant than benign lesions had washout curves.
"We found that in the largest database of lesions imaged with the older protocol and system 1 ... most of the malignant lesions were classified as washout, whereas persistent was the most likely descriptor of benign lesions," the authors wrote. "Most malignant lesions imaged with protocol and system 2 also were classified as washout, but only 19% of benign lesions were classified as persistent. More important, with imaging protocol and system 3, fewer than one-half of kinetic curves of malignant lesions were classified as washout."
 |
| Contrast enhancement of malignant lesions. Graphs show percentage of lesions with BI-RADS descriptor of kinetic curve shape during initial rise (A) and delayed phase (B) on MR images acquired with imaging protocols and systems 1, 2, and 3. |
Differences in average kinetic parameters across the three protocols and systems could be caused by a number of factors, Jansen and colleagues wrote, including k-space sampling, T1 weighting, and magnetization transfer effects.
Whatever the reason, clinicians need to keep in mind that these inconsistencies could create problems: For example, in follow-up MRI of women undergoing preoperative neoadjuvant chemotherapy, it would be important to perform follow-up imaging with the system used initially, so that any differences due to system choice wouldn't be mistaken for tumor response.
"The results of this study emphasize the importance of standardization of dynamic contrast-enhanced MRI acquisition protocols so that as newer technology is implemented, malignant lesions are sufficiently conspicuous and similar interpretation guidelines can be consistently applied across all systems and protocols," the authors concluded. "Such standardization is important if breast dynamic contrast-enhanced MRI is to be used routinely in patient care."
By Kate Madden Yee
AuntMinnie.com staff writer
August 25, 2009
Related Reading
Kinetic information identifies MRI-detected breast tumors, August 19, 2009
Study: MRI may cause more harm than good in breast cancer, August 13, 2009
PET/MRI breast imaging prototype shows early promise, June 16, 2009
Molecular breast imaging offers promise as mammography adjunct, September 15, 2008
Open-source software delivers 3-way (PET/CT/MR) image fusion, April 25, 2008
Copyright © 2009 AuntMinnie.com

















