Radiation dose measured at the skin is higher and overall effective doses more variable with conventional angiography compared to coronary CT angiography (CTA), say researchers from the Medical University of South Carolina (MUSC) in Charleston. In fact, some skin doses at angiography were so high as to risk skin burns; on the other hand, many of the procedures in the patient cohort were particularly complex.
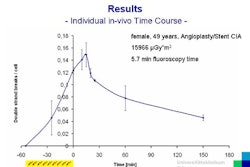
"The purpose of our study was to directly compare patient radiation doses at coronary CTA compared with those of invasive angiography [ICA]," said Dr. Alexander Sterzik in a presentation at the 2009 European Congress of Radiology (ECR).
Sterzik and his MUSC colleagues, including Dr. Joseph Schoepf and Walter Huda, Ph.D., quantified effective doses in dose length product (DLP) converted to mSv, a dose measure that can be used to estimate the stochastic risk of cancer and genetic mutations, while allowing for direct comparison across different radiologic modalities, Sterzik said.
A total of 104 consecutive patients underwent coronary CTA on a 64-detector-row CT scanner (Sensation 64, Siemens Healthcare, Malvern, PA). Effective radiation dose was quantified using DLP measurements, and average skin organ dose was quantified using the CT dose index volume (CTDIvol) and converted to mGy-cm. The conversions were based on a paper by Huda et al (Radiology, September 2008, Vol. 248:3, pp. 995-1003), Sterzik said.
A second group of 102 consecutive patients underwent conventional angiography. Data were obtained on the basis of a point reference dose 15 cm from the isocenter and the number of runs, fluoroscopy time, and kerma-area product (KAP). To estimate skin dose, CTDIvol was multiplied by 2.5, Sterzik said.
The mean DLP for coronary CTA was 1,120 ± 200 mGy-cm with an average effective dose equivalent to 21 mSv. For conventional angiography, the mean number of imaging runs was 12.2 ± 7.6 and the mean fluoroscopy time was 9.9 ± 11.5 minutes. Average KAP was 84.1 ± 83.7 Gy-cm2 with an average effective dose equivalent to 15 mSv.
"The average effective dose at coronary CTA was in the range of 21 mSv, compared to invasive coronary angiography at 15 mSv," Sterzik said. "However, the skin as well as the effective doses in the invasive angiography group are subject to much greater variability [at ICA]. This is reflected in the coefficient variation, which was in the range of 100% for invasive angiography versus about 20% for coronary CTA."
For all studies the median CTDIvol was 58 mGy, and at the 10th and 90th percentiles median, CTDIvol was 58 mGy and 69 mGy, respectively, the authors reported in an abstract. For coronary CTA, the skin dose was approximately 2.5 times higher than CTDIvol, with an estimated corresponding skin dose of approximately 150 mGy.
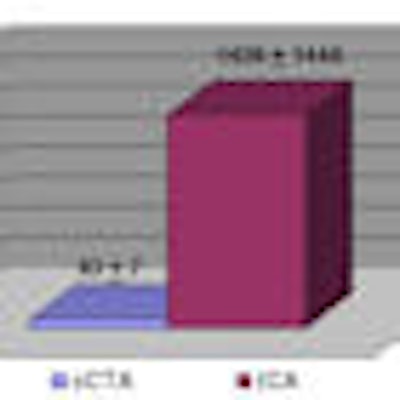
At angiography, the average reference point dose -- the dose measured at the point where the x-ray beam enters the patient's body -- was 1,420 ± 1,440 mGy, with a median reference point dose of 960 mGy and 10th and 90th percentiles at 300 and 2,940 mGy, respectively. At coronary CTA, the average reference point dose was 63 ± 7 mGy.
 |
| The average dose at the point where the x-ray beam enters the body (average reference point dose) was much higher for ICA (1,420 ± 1,440 mGy) than for coronary CTA (63 ± 7 mGy). Image courtesy of Dr. Alexander Sterzik and Dr. Joseph Schoepf. |
"In our patient collective, the skin doses in invasive angiography were about 10 times higher than that of coronary CTA," Sterzik said. "And in 20% of the patients, the skin dose exceeded 2,000 mGy, which is the threshold dose at which ... effects such as skin burns can occur."
Coronary CTA doses weighed in slightly higher than those of invasive angiography, 21 versus 15 mSv, "but, of course, the variations for skin doses as well as the effective doses in invasive angiography were much more pronounced than for coronary CTA," he added.
No breast shields were used in the study, Sterzik said in response to a question from the audience. The relatively high doses reported for both modalities can be explained by the complexity of procedures and settings in which ICA and coronary CTA were used.
For ICA in the setting of coronary artery bypass graft (CABG) surgery, "you automatically get high doses," he said. At coronary CTA, patients were being evaluated for chest pain and "for the patency of CABG, which requires [long] scan lengths," he said.
By Eric Barnes
AuntMinnie.com staff writer
May 4, 2009
Related Reading
Tube current modulation cuts triple rule-out CTA dose, April 15, 2009
320-detector-row CT cuts dose in triple rule-out exams, February 12, 2009
AHA science advisory warns about cardiac imaging dose, February 3, 2009
JAMA study finds wide variation in cardiac CTA dose, February 3, 2009
MDCT for chest pain: Whom to scan, when to discharge, August 22, 2008
Copyright © 2009 AuntMinnie.com