In another side benefit to CT colonography screening, researchers have discovered that the technique can measure abdominal aortic calcification, which could be more effective than traditional measures for estimating a person's risk of heart attack, death, and other cardiovascular events, according to an October 2 article in Radiology.
Researchers from the University of Wisconsin and the Medical College of Wisconsin used calcium scoring software to measure the degree of abdominal aortic calcification on CT colonography (CTC) scans of individuals undergoing colon cancer screening. They determined that a high aortic calcium score had a statistically significant correlation with future adverse cardiovascular events.
What's more, the predictive capacity of abdominal aortic calcification on CTC topped that of the long-established Framingham risk score for estimating future cardiac events.
"We found a strong association between abdominal aortic calcification and future cardiovascular events," first author Dr. Stacy O'Connor said in a statement. "With heart disease being a leading cause of death, anything we can do to make our patients more aware of their risk is going to help."
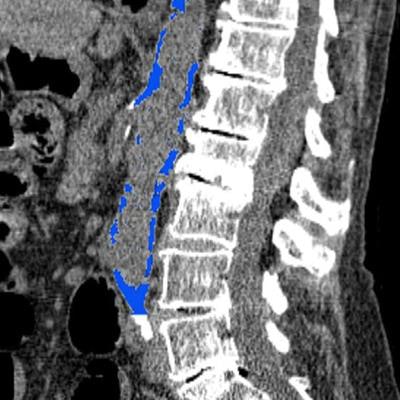
 CT colonography scan showing abdominal aortic calcification (blue). Image courtesy of RSNA.
CT colonography scan showing abdominal aortic calcification (blue). Image courtesy of RSNA.Predicting cardiovascular events
The most widely used model for predicting an individual's 10-year probability for a cardiovascular event is the Framingham risk score, which takes into account traditional risk factors such as age, smoking history, cholesterol levels, and blood pressure. High Framingham risk scores can help clinicians identify patients who most likely require treatment to prevent a cardiovascular event.
A downside of the standard Framingham method is that it occasionally categorizes individuals as having indeterminate risk, the authors noted. More comprehensive risk evaluation for these individuals often requires an additional noninvasive test capable of providing information on other independent risk predictors, such as plaque buildup in the coronary arteries.
Investigating the potential of CT colonography to fit the bill, O'Connor and colleagues evaluated the scans of 829 people who underwent CT colonography screening between April 2004 and March 2005. They followed the cohort for an average of 11 years after screening to confirm the occurrence of any cardiovascular events. In total, there were 156 adverse cardiovascular events, including heart attack (5%), stroke (3%), and death (10%).
The researchers used a semiautomated CT software tool (V3D-Calcium Scoring, Viatronix) to segment and quantify abdominal aortic calcification on the CT colonography scans.
On average, they discovered that calcification in the abdominal aorta was more than five times higher for individuals who had a cardiovascular event than for those who did not experience an event (calcium score of 3,478 versus 664, p < 0.001). Thus, abdominal aortic calcification on CT was a statistically significant predictor of cardiovascular events -- better even than the Framingham risk score.
| Framingham risk score vs. CTC calcium score for predicting cardiac events | ||
| Area under the curve | Framingham risk score | Abdominal aortic calcification on CT colonography |
| 2-year risk* | 0.64 | 0.82 |
| 5-year risk | 0.64 | 0.75 |
| 10-year risk* | 0.67 | 0.76 |
Furthermore, the rate of cardiovascular events increased in accordance with increasing calcium scores: 4% of individuals in the lowest quartile of calcium scores had a cardiovascular event, compared with 12% in the second quartile, 18% in the third quartile, and 41% in the highest quartile.
'Opportunistic measures'
Abdominal aortic calcification measurements may not only facilitate cardiovascular disease prediction but also improve patient care as well, O'Connor and colleagues noted. They determined that using a threshold calcium score of 200 on CT colonography improved an individual's risk categorization by 35.4% for 10-year risk, compared with the Framingham risk score. Thus, individuals with a high abdominal aortic calcification score may require aggressive preventive treatment, even if their Framingham risk score indicates otherwise.
Although these findings demonstrate the benefits of measuring abdominal aortic calcification on CT, the researchers do not necessarily support the idea of acquiring an abdominal CT scan solely to screen for cardiovascular risk. Rather, they believe the results add to the growing list of advantages of using abdominal CT exams such as CTC to screen for colorectal cancer and other diseases.
For example, clinicians may be able to use calcification measurements to address cardiovascular concerns for a patient already scheduled to undergo an abdominal CT scan for, say, a gallbladder infection, without the need for additional testing, the authors noted.
"There are thousands of CT scans performed every day across the United States, so this gives us an opportunity to reach a lot of people," O'Connor said. "It's our hope that these opportunistic measures can be added to reports for patients undergoing routine abdominal CT, regardless of the imaging indication."
Looking ahead, the researchers plan to build upon their results by conducting a similar study in a larger population. They also intend to move toward a fully automated protocol for more widespread implementation of the assessment.


















