
Conventional axial CT scans may not be up for the job of detecting all pulmonary nodules, but maximum intensity projection (MIP) postprocessing can lend a much-needed helping hand, Australian researchers have found.
In a retrospective study, researchers from Southern Health Network in Melbourne found that multiplanar MIP was able to improve upon the performance of conventional axial 5-mm exams, which missed 40% of pulmonary nodules in a retrospective study. Although more time consuming, the combination of MIPs in all three imaging planes with a slab thickness of 5 mm yielded 94% sensitivity and 96% positive predictive value, said Dr. Zhi-Yie (Judith) Tan.
She presented the research during a session at last week's American Roentgen Ray Society (ARRS) meeting in Vancouver.
Small pulmonary nodules are common: 88% to 97% of nodules found in lung cancer screening studies are 10 mm or smaller, according to Tan. While previous studies have found that CT exams that received maximum intensity projection (MIP) postprocessing are more sensitive for detecting nodules than those without it, there has been limited assessment of MIP variations, as well as limited comparisons with conventional axial thin slices, computer-aided detection (CAD), and volume rendering, according to Tan.
As a result, the researchers sought to evaluate the efficacy of CT detection of pulmonary nodules by using MIPs of different slab thicknesses and different scan planes. In a retrospective review, 72 consecutive thoracic CT patients were studied from Monash Medical Centre from February to March 2010. The patients included 25 females and 47 males with a mean age of 57 (range, 2-91 years).
Four different MIP slab thicknesses (2.5 mm, 5 mm, 7.5 mm, and 10 mm) were reconstructed from CT data in axial, sagittal, and coronal planes. Blinded to the patients, slab thickness, and number of reported nodules, two radiologists independently evaluated the images for presence, size, and location of pulmonary nodules.
The researchers then compared their results with findings on the conventional axial 5-mm CT studies. A consensus panel had determined there were 154 "true" nodules based on all available CT series with the aid of prior and follow-up CTs in most patients, according to the study team. The nodules had a size range of 0.5 mm to 23 mm, with a median of 2.5 mm and a mean of 3.5 mm; 93% were peripheral, while 7% were central.
Of the 154 pulmonary nodules, 61 (40%) were missed on conventional axial CT. These nodules had a size range of 1 mm to 6 mm and median and mean size of 3 mm.
 |
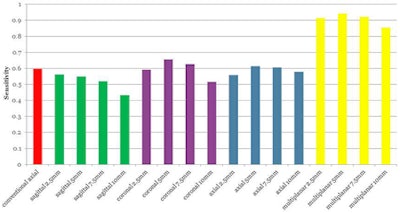
| Sensitivity for CT detection of pulmonary nodules with different slab thicknesses and scan planes using single- and multiple-plane assessment, compared with nonpostprocessed 5-mm axial images. All images courtesy of Dr. Judith Tan. |
As for individual planes, coronal 2.5-mm MIP yielded the highest positive predictive value (99%), while coronal 5-mm MIP had the highest sensitivity (66%). When combining MIP from all three planes, the 5-mm slab thickness yielded the best pulmonary nodule detection performance: 94% sensitivity and 96% positive predictive value.
The researchers also assessed the ability of MIP to identify patients with at least one pulmonary nodule.
"This is because in our institution these patients often receive further attention, either in the form of a follow-up CT examination and/or referral to a respiratory physician (pulmonologist)," Tan said. "[In these patients], there was improvement in sensitivity and positive predictive values, a consistent finding across different slab thicknesses and scan planes, using MIPs compared with conventional axial 5-mm CT."
 |
| Sensitivity for CT detection of nodule-positive patients with different slab thicknesses and scan planes using single- and multiple-plane assessment, compared with nonpostprocessed 5-mm axial images. |
Individual nodule detection with single-plane MIP is not significantly different than conventional axial CT, but it does have a slight advantage in identifying patients with one or more nodules, according to the researchers.
"Multiplanar MIP assessment improves CT detection of pulmonary nodules; however, single-plane MIP may improve identification and follow-up of patients with nodules," Tan told AuntMinnie.com.
In other findings, the researchers noted that nodules were more likely to be missed on conventional axial CT as the distance increases from the lung periphery. Of the 10 nodules more than 3 cm from the lung periphery, seven (70%) were missed by conventional axial CT. Ten (43.5%) of the 23 nodules 2 cm to 3 cm from the periphery were missed, as were 16 (45.7%) of the 35 nodules 1 cm to 2 cm from the periphery. Twenty-five (30.5%) of the 82 nodules less than 1 cm from the periphery were missed.
Excellent inter-reader agreement was also seen over the varying MIP slab thicknesses, according to Tan.
Inter-reader agreement for MIP interpretation
|
The researchers acknowledged limitations of their study, including the lack of a true histopathologic standard. In the study, 57% of the patients had a previous or subsequent CT that was available for comparison.















