Radiation dose from CT can be reduced significantly, according to a pair of articles in the current issue of the Journal of the American College of Radiology. The articles provide tips on topics ranging from technical scanning parameters to staff training and quality control.
In the first article, researchers from Massachusetts General Hospital, Harvard Medical School, and Johns Hopkins University examined methods for reducing dose in the head, paranasal sinuses, and spine. They emphasized the use of techniques such as lower tube current, automatic exposure control, and reduced tube voltage as key to substantially reducing dose for head CT examinations in both children and adults.
Despite the increasing use of MRI when possible, CT remains an important tool, particularly for cerebrovascular diseases and head trauma, wrote Mahadevappa Mahesh, PhD, and colleagues (JACR, August 2011, Vol. 8:8, pp. 591-593).
In children, for example, MRI is increasingly sought for head imaging, but CT is still preferred for certain indications such as acute trauma, stroke, hydrocephalus, and craniosynostosis.
To optimize radiation dose, specific scanning protocols must be assigned depending on the examination type or clinical indication, such as routine head CT, CT angiography, CT perfusion, or paranasal or facial CT, Mahesh said in a statement about the study.
To ensure that the protocols are used as designed, scanning techniques must be saved on the scanner user interface or explicitly documented in some form to avoid guesswork and potential errors at the time of imaging, the authors wrote.
Studies have shown that adult head CT radiation dose can be reduced by lowering tube current as much as 50% with acceptable noise levels and differentiation of gray and white matter.
Another promising dose-cutting approach, the use of iterative reconstruction techniques to enable dose reduction for chest and abdominal CT, has not been reported for head CT, they noted.
In pediatric CT, children's thinner skulls mean that dose can be reduced even further (e.g., 80 kVp, 50 mAs) to obtain required diagnostic information at radiation doses of fractions of a millisievert, according to the authors. Optimal dose reduction is even more critical in applications such as shunt patency studies in children with ventriculoperitoneal shunting, who often undergo multiple repeat exams.
 |
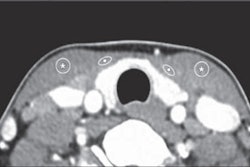
| Low-dose craniosynostosis CT protocol in a 1-year-old girl revealed telecanthus but no craniosynostosis. Scan parameters of 80 kVp and 50 mA resulted in an estimated effective radiation dose of 0.1 mSv. Images republished with permission of the American College of Radiology from JACR, August 2011, Vol. 8:8, pp. 591-593. |
"Because perfusion CT imaging involves multiple repeat scanning at the same location, unless scanning parameters are modified appropriately compared with routine head CT parameters, radiation doses can reach levels exceeding the threshold to induce deterministic adverse effects such as hair loss," Mahesh and colleagues wrote, stating that tube current must not exceed 80 kVp for this application.
Dose reduction in community hospitals
The second JACR article reported on CT dose reduction in small and medium-sized hospitals, in a study authored by Mary Ellen Jafar and Dr. Lonnie Simmons from Gundersen Lutheran Health System in La Crosse, WI (pp. 588-590).
Their recommendations include the following components:
- Develop optimized CT acquisition protocols for reduced radiation, while maintaining adequate image quality. Key protocols include coronary CT angiography, low-dose renal stone scans, CT topographic bone growth, CT neck soft-tissue, and low-dose scans for spondylolysis patients.
- Ensure proper CT scanner functionality by performing acceptance testing on each scanner at installation. CT technologists and physicists should perform regular quality control testing based on the American College of Radiology's technical standard for diagnostic medical physics performance monitoring of CT equipment.
- Ensure appropriately trained staff members meet state regulatory requirements and, if employed by an accredited facility, fulfill accreditation body requirements for initial qualification, continuing education, and continuing experience.
- Staff should also regularly monitor radiation doses and work to educate referring physicians, according to the authors.
In addition, new dose reduction technologies from manufacturers are important in scanner selection, Jafar and Simmons wrote.
These technologies include attenuation-dependent tube current modulation; automatic exposure control; noise-reducing, resolution-preserving image reconstruction methods (multidimensional adaptive filtering); anatomy-adapted tube current modulation; dynamic collimation to reduce overscanning effects; automatic tube voltage selection; availability of lower tube voltage selection; and dual-energy imaging functionality.