Cardiac MRI may be the gold standard for evaluating myocardial perfusion, but there's no reason CT can't eventually take over much of MRI's workload in patients suspected of coronary artery disease, say researchers from the Medical University of South Carolina (MUSC) and two other centers.
CT is used mainly for evaluating the coronary arteries and is not the primary method of evaluating myocardial perfusion. But if the modality demonstrates its effectiveness for perfusion imaging, it could replace physiological tests, enabling radiologists to use a single modality for comprehensive cardiac imaging.
Indeed, the researchers found that single-scan dynamic stress perfusion CT provides a comprehensive evaluation of coronary artery disease comparable to stress/rest perfusion MRI and delayed-enhancement MRI. CT showed high sensitivity for the detection of perfusion defects, making it an attractive solution for integrated imaging of anatomy, function, perfusion, and viability.
Adenosine-stress first-pass myocardial CT perfusion imaging enables the evaluation of qualitative and semiquantitative parameters of myocardial perfusion in a comparable fashion as MRI, and may enable absolute quantification of myocardial blood flow, said MUSC's Markus Weininger, MD, in a presentation at the 2010 RSNA meeting.
Limited for morphology?
CT has, of course, amply demonstrated its ability to rule out significant coronary artery stenosis. But in its current form, cardiac CT's diagnostic value for evaluating the functional significance of stenosis remains limited due to its restricted ability for dynamic evaluation of the contrast medium's passage through the myocardium, he said.
"CT's strict morphological evaluation is incomplete for comprehensive assessment of all aspects of coronary artery disease, but advances in CT technology have made it feasible for CT to evaluate all aspects of coronary artery disease, including a detailed morphological assessment of the coronary arteries, and a hemodynamic evaluation of detected stenoses," Weininger said.
The study, from MUSC as well as Ajou University Hospital and the University of Navarra, aimed to evaluate the feasibility of adenosine-stress myocardial perfusion imaging using second-generation dual-source CT for the qualitative and quantitative assessment of myocardial blood flow (MBF) compared to MRI.
In the study, 20 patients (six female; mean age, 60 ± 11 years) underwent a standardized cardiac three-phase dual-energy CT protocol (Somatom Definition Flash, Siemens Healthcare). Imaging consisted of prospectively electrocardiogram (ECG)-triggered coronary CT angiography, dynamic adenosine-stress myocardial perfusion imaging using "shuttle" mode on the scanner, and delayed-enhancement acquisitions.
The scanner's shuttle mode acquires data during every other RR interval at two alternating table positions with ECG triggering, with the table shuttling back and forth between the two positions during image acquisition.
- The end-systolic acquisition was performed three minutes after administration of adenosine stress (140 µg/kg/min) using a dynamic acquisition mode at two alternating table positions.
- The sequence began four seconds prior to the front arrival of the bolus, ensuring baseline acquisition of noncontrast images (100 kV, 300 mAs, 50 mL contrast and 50 mL saline chaser at 6 mL/sec flow rate).
- Image reconstruction included 3-mm slice thickness every 2 mm, resulting in a mean dose-length product of 733 mGy.
Patients also underwent stress and rest/perfusion MRI and delayed-enhancement MRI. Two independent observers blinded to the results visually assessed myocardial perfusion defects.
 |
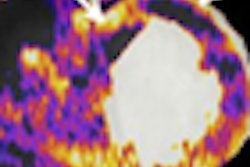
| Above, 50-year-old man presenting with chest pain underwent stress myocardial perfusion SPECT and CT, which showed corresponding areas of perfusion defects, as did MRI. Right, patient underwent cardiac catheterization for stenoses in the left anterior descending and right coronary arteries. All data and images courtesy of Markus Weininger, MD. |
 |
| In a 61-year-old man with suspected coronary artery disease, myocardial stress perfusion CT (a, b) reveals hypoperfused regions corresponding to SPECT (c) and MRI (d) studies. |
For semiquantitative evaluation, the authors compared CT- and MRI-derived myocardial-to-left-ventricular upslope indices using software (Argus, Siemens Healthcare) analysis of short-axis reformats.
 |
| In semiquantitative analysis, both CT (above) and MRI (below) showed significant differences in upslope of signal intensity over time curve. |
 |
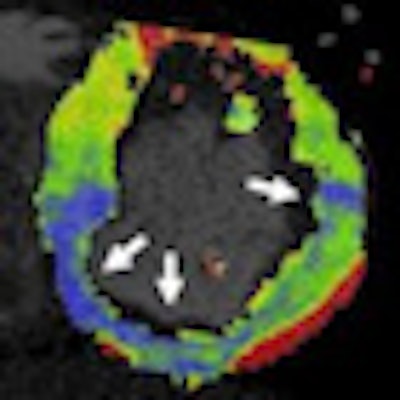
Finally, absolute myocardial blood flow was quantified based on dynamic perfusion CT and correlated with semiquantitative CT measurements using a prototype software application (syngo Volume Perfusion, Siemens Healthcare). Here, CT was able to identify differences in myocardial blood flow between normal and ischemic myocardium.
 |
| There was a significant difference in myocardial blood flow between normal and hypoperfused myocardium (p < 0.001). Moderate correlation was found between absolute myocardial blood flow quantification and the upslope of signal intensity over time curves (r = 0.47, p < 0.01). There was also moderate correlation between myocardial blood flow and semiquantitative upslope for hypoperfused and normal myocardium (r = 0.41, p < 0.01 vs. r = 0.43, p < 0.01). |
Statistical analysis was performed using paired t-tests, Wilcoxon signed-rank test, linear correlation, and Bland-Altman statistics.
CT perfusion correctly classified 54 perfusion defects, demonstrating a sensitivity of 86%, specificity of 98%, positive predictive value of 93%, and negative predictive value of 94%, Weininger said.
Diagnostic performance of CT, MRI for myocardial perfusion
|
"Adenosine-stress dynamic myocardial perfusion CT is technically feasible and can differentiate between healthy and diseased myocardium," Weininger said. "It allows evaluation of qualitative and semiquantitative parameters comparable to MRI, and it's particularly promising for absolute quantification of myocardial blood flow, though there is only moderate correlation with the upslope of the signal intensity over time curve."
"CT is an attractive modality for integrative imaging of anatomy, function, perfusion, and viability," he said. "The final question is, when it will replace traditional physiological testing?"