A study boasting an unusually long follow-up period found that chest pain patients without significant stenoses at coronary CT angiography (CCTA) had no cardiac events, deaths, or interventions within three years of being scanned.
And because patients with negative coronary CTA results could be safely discharged, the CT strategy was found to cost far less than the standard of care: about $5,000 per patient versus five times as much for stress tests followed by invasive angiography.
"Despite the numerous publications verifying the exceptional diagnostic performance of CCTA in detecting high-grade [coronary artery disease (CAD)], this test has yet to be universally adopted by healthcare providers or by third-party payors," wrote Dr. Poorya Fazel and colleagues. "One of the main reasons that this has not yet occurred is that the durability of those findings over a prolonged duration has yet to be confirmed" (American Journal of Cardiology, August 15, 2009, Vol. 104:4, pp. 498-500).
The researchers aimed to evaluate the long-term clinical utility of 64-detector-row coronary CTA in patients with chest pain -- some with and some without previous abnormal stress tests -- who had a low-to-intermediate pretest probability of flow-limiting CAD. The group from Baylor University Medical Center in Dallas also analyzed the costs of care to determine if CTA was cheaper over time.
The study included 436 consecutive patients (97 men, ages 18 to 77 years; mean age, 53 ± 11; 239 women, ages 30 to 79 years; mean age, 56 ± 11) diagnosed with chest pain. All underwent 64-detector-row coronary CTA following the administration of beta-blockers to achieve a heart rate of 65 beats per minute or less, and IV administration of iodinated contrast. Patients were scanned using a retrospective triggering technique (mean radiation dose, 12 mSv) on a 64-detector-row LightSpeed VCT scanner (GE Healthcare, Chalfont St. Giles, U.K.).
"All patients presented with chest pain concerning for angina, but it was thought that initial referral for invasive evaluation was unnecessary," Fazel and colleagues wrote. "Individually, these patients were considered by their referring physician to be at lower risk for significant, flow-limiting CAD based on their age, lack of risk factors, or quality of their chest pain."
Among the subgroup of patients who had undergone stress testing, many were referred because their findings were equivocal or felt to be more consistent with a false-positive stress test result (e.g., greater than 1-mm ST depression at peak exercise with good exercise capacity and no wall motion abnormalities, or ischemic defects on imaging). However, additional coronary evaluation was considered necessary in every case.
"The decision to proceed to CCTA rather than invasive angiography was made at the discretion of the treating cardiologist and was typically based on a continued belief that the patient was not high risk for flow-limiting CAD," the authors wrote. In this subgroup, 17 patients proceeded to coronary catheterization and seven patients ultimately underwent percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG).
Follow-up information on the occurrence of coronary catheterization, coronary revascularization, nonfatal myocardial infarction, and death was obtained by reviewing patient charts and examining medical records, including the national death database, from the time of the scan through May 2008.
Referrals for coronary CTA were included only if the patient had an initial diagnosis of chest pain, and patients with a history of PCI or CABG were excluded.
Of the 436 total patients, 376 had no significant coronary artery disease based on the coronary CTA results. Of the 60 patients who were considered to have flow-limiting CAD, 57% (n = 34) went on to have PCI or CABG within the follow-up period, representing true positives at CTA.
Most patients were scanned with coronary CTA as their first test, but 78 (18%) patients had a stress test before CT.
No stress tests had a "strongly positive stress test result suggestive of left main or multivessel CAD," the group wrote.
 |
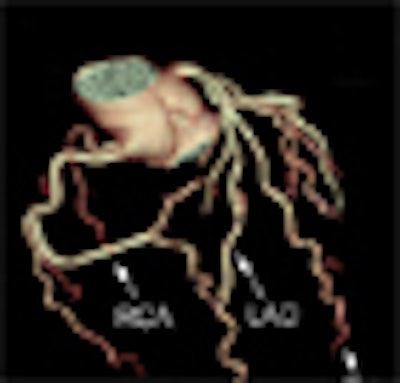
| A 40-year-old with risk factors for CAD and chest pain, worrisome for angina. Image demonstrates (A) 3D rendering of a right-dominant heart with (B) axial views of the left main artery, proximal left anterior descending (LAD) artery, and proximal right coronary artery (RCA) showing no plaque. Multiplanar reformatted views of the LAD (C) and RCA (D) also show no disease. Images courtesy of Dr. Jeffrey Schussler and Dr. Poorya Fazel. |
Patients were considered true negative at coronary CTA if they did not return for care over the mean three-year follow-up with a cardiac event or a need for further testing. During this period, no patient with minimal or no atherosclerotic CAD at coronary CTA suffered a cardiac event, required intervention, or died from cardiovascular disease, the group reported. The coronary CTA results were as follows:
- Sensitivity 26/26 (100%)
- Specificity 376/402 (94%)
- Positive predictive value 34/60 (57%)
- Negative predictive value 376/376 (100%)
Cost analysis
The actual costs for coronary CTA and catheterization varied depending on the healthcare payor, the authors wrote. The study assumed a cost of $2,000 per coronary CTA study and $8,000 per invasive angiography, a standard that tended to "overestimate the cost of the noninvasive test and underestimate the cost of diagnostic angiography."
Based on these assumptions, estimated costs were $318,225 ($5,217 per patient) for patients undergoing only coronary CTA and $415,225 ($24,425 per patient) for those undergoing angiography.
"Traditionally, all patients who initially underwent stress testing, but in whom further evaluation was warranted, would have proceeded with invasive evaluation," Fazel and colleagues wrote. "The estimated total cost would equal approximately $1,653,600 ($21,200/patient). The cost difference between the direct catheterization group and the groups using CCTA was approximately $919,650 in favor of the CT groups."
By Eric Barnes
AuntMinnie.com staff writer
August 26, 2009
Related Reading
Coronary CTA beats calcium scoring for short-term prognosis, August 14, 2009
DECT cuts tests as a one-stop myocardial, coronary artery exam, August 10, 2009
Lower-kilovoltage coronary CTA maintains image quality, August 5, 2009
Dual-source CTA turns in mixed results for coronary stenoses, July 30, 2009
CTA predicts coronary plaque instability, June 30, 2009
Copyright © 2009 AuntMinnie.com