Two studies presented on Monday at the 2008 American College of Cardiology (ACC) meeting in Chicago are emblematic of a new wave of evidence supporting the first-line use of CT in subjects with and without suspected heart disease.
Physicians using cardiac CT give it high marks for reigning in costs, speeding throughput, improving care, and even eliminating some costly exams in the standard cardiac workup. To date, few studies have been available to support the anecdotal enthusiasm. But the situation is changing as new research illuminates CT's advantages compared to traditional workup strategies in patients at risk of coronary artery disease.
In the studies presented Monday at the Chicago meeting, researchers from the Los Angeles Biomedical Research Institute at Harbor-UCLA (University of California, Los Angeles) in Torrance, CA, found measurable benefits when their standard workup protocols were replaced with cardiac CT.
First, a study led by the institute's Dr. Nicole Weinberg examined the use of cardiac CT as a gateway to cardiac catheterization in 495 asymptomatic firefighters. Using gated coronary CT calcium scans, the researchers were able to effectively triage the subjects into follow-up cardiac CT angiography (CTA) -- or send them back to work without further workup.
In a second study, researchers led by Dr. Ronald Karlsberg, the cardiology program director at Harbor-UCLA Medical Center, integrated coronary CTA into an office-based cardiology practice. Incorporating coronary CTA reduced the need for myocardial perfusion imaging and exercise treadmill testing. Moreover, doctors were able to identify more coronary artery disease and provide more aggressive lipid management, while keeping office income relatively stable.
Participating in both studies was Dr. Matthew Budoff, an associate professor of medicine at UCLA and director of cardiology at Harbor-UCLA Medical Center. Budoff discussed the research with AuntMinnie.com.
Putting out fires
Firefighting is known as a high-risk profession, but not all of the risks are obvious. Take heart disease. A 2005 survey by the National Fire Protection Association revealed that 43.7% of deaths among active firefighters between 1995 and 2004 were from sudden cardiac death, including coronary artery disease.
Hoping to reduce the death toll, both the city and county of Los Angeles operate programs to screen firefighters before they are assigned to active duty. The departments have entered into contracts with Harbor-UCLA to screen every firefighter in Los Angeles as part of a work-fitness assessment.
"We use (CT) a lot for firefighters because it expedites patient care," Budoff said.
Before the scanning component was added to the workup, Los Angeles firefighters would obtain an annual treadmill test to assess fitness for duty and screen for heart disease, he explained. If a treadmill test was positive, the firefighter was relieved of duty and replaced with another firefighter until the primary firefighter could be evaluated by a cardiologist and cleared for duty, which generally required two to three weeks.
With the addition of CT, the whole screening process is faster now, Budoff said. Firefighters with abnormal treadmill results are examined with a gated coronary calcium scan. Those with calcium scores of 10 or less are sent back to work. Those with scores higher than 10 are referred for coronary CTA. Most of these are also negative, and are sent back to work.
"Treadmill as a first-line test is a little problematic," Budoff said. "Only about 70% of the results are accurate." Not only is it limited to detecting fairly high-grade stenosis, but it yields a substantial number of false positives. For the firefighters, "it's more of a fitness-for-duty test than a cardiac assessment," he said.
 |
| About 16% of firefighters with calcium scores greater than 10 were referred for coronary CTA. Among the patients undergoing CTA, 40 of the 133 (30%) of patients had significant coronary artery disease. All images courtesy of Dr. Matthew Budoff. |
The average radiation dose for the gated calcium scans is 0.7 mSv, compared to 4.2 mSv for coronary CTA. About 70% of CTA exams were performed using a prospectively gated protocol (SnapShot Pulse, GE Healthcare, Chalfont St. Giles, U.K.). The rest underwent retrospectively gated triphasic exams with dose modulation. At this time, approximately 90% of CTA exams are performed with prospective gating, yielding an average radiation dose of 2.4 mSv per scan.
Harbor-UCLA researchers have so far examined 495 generally active and healthy firefighters between the ages of 40 and 65 years with positive or equivocal treadmill stress tests using a gated calcium scoring scan.
 |
| Coronary artery calcium scans were performed on a 64-detector-row scanner using 3-mm contiguous scans from the carina to the apex of the heart, with ECG triggering of 60% to 70% of the RR interval. |
According to the results, 57% (281) of the 495 subjects had calcium scores of zero, and 16% (81) had scores of 1 to 9 and returned to work immediately after being counseled about the implications of coronary artery calcium. Those cleared to go back to work have had no negative outcomes over the three-year follow-up period, Budoff noted.
Another 133 firefighters had a positive CTA exam showing at least one coronary artery stenosis of 50% or greater. These workers were put on restricted duty and scheduled for cardiac catheterization for further management.
"We found critical, multivessel disease that required urgent surgery in a couple of cases," Budoff said.
 |
| A 52-year-old firefighter with abnormal treadmill results underwent gated coronary calcium scan demonstrating a score of 132. The subject then underwent coronary CTA, which demonstrated a stenosis of approximately 70% in the midleft anterior descending artery. After percutaneous transluminal angioplasty and stenting the patient returned to work. |
When the study was designed, prospectively gated CTA wasn't available yet, so it made sense to start with gated calcium scoring in firefighters who failed the treadmill test, since the radiation dose is substantially lower than for retrospective gating, Budoff explained. However, "now that CTA is almost the same radiation dose, we can move toward more CTA in this cohort," he said. Firefighters tend to be young, healthy, and active, therefore a "great group" for prospectively gated CTA, Budoff said. "We'll shift away from calcium scoring as we get SnapShot Pulse better established."
In Budoff's view, the firefighter screening program has been a resounding success. "We're happy, and the fire department is very happy because the vast majority of firemen are back to work within an hour, whether it's calcium (scoring) or calcium plus CT angiography," he said.
Integrating cardiac CTA
In the ACC study led by Karlsberg, coronary CTA cut the number of heart exams and reduced costs when it was introduced in a 17-member office-based cardiology practice in 2006.
"Since CTA was introduced, what we've experienced in practice is both a definitive decrease in nuclear testing as well as standard treadmill testing in both six-month periods that we evaluated," Budoff told AuntMinnie.com. "We've also seen a decrease in normal cardiac catheterizations and a slight decrease in angioplasties and stenting."
After installing a 64-slice CT scanner (LightSpeed VCT, GE) and using it for a year, the group compared exam volumes from the six-month period before the study began to the first six months and the last six months of the one-year study period.
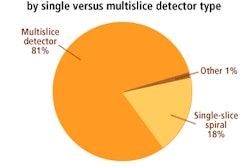
They performed a total of 3,972 CT studies on 3,468 patients during 2006, their first year of operation. Overall, 18% of the scans were gated coronary artery calcium studies, 36% were coronary CTA (n = 1,412), and 45% were noncardiac CT (n = 1,770). IV contrast was used in 52% of the studies (n = 2,054), the authors noted in an abstract.
Most patients can be scanned at 100 kVp, Budoff said. Generally, those weighing more than 85 kg (187 lb), approximately a fifth of patients being evaluated, must be imaged at 120 kVp. Reconstructions in the form of maximum intensity projections (MIPs) and multiplanar reformations (MPRs) are read on a GE Advantage workstation.
Compared to the prior six months, during the first six months after CTA integration, the number of SPECT myocardial perfusion imaging exams dropped by approximately 15% (1,682 versus 1,442 studies, p < 0.01), according to the study authors. The reduction was sustained for the second six months as well, during which a total of 1,422 SPECT exams were performed.
The exercise echocardiography volume of 531 exams increased slightly during the first six months of the study period (to 560 studies) and the second six months (589 exams, p < 0.05). The standard treadmill testing volume of 240 exams also dropped during both six-month study periods (124 and 149 respectively, p < 0.01).
"The normal CTA is pretty definitive," Budoff said. "We're pretty comfortable with the high negative predictive value of 99%, and we don't feel those patients deserve further imaging if their CTA is normal, so they don't go on to further stress echo or stress nuclear studies, and we stop with (CTA)."
CTA's negative predictive value leads to fewer cardiac catheterizations, Budoff added, because if it's a normal CTA, the borderline nuclear cases no longer need to go to the cath lab, further reducing costs.
How did the utilization changes affect practice revenues? "Net office income did not decrease significantly," Budoff said. "There was a slight, not statistically significant, overall decline in payroll from interventions, but net office income did not decline significantly."
Budoff believes that assessing income can be a bit challenging. A highly accurate assessment would have required accounting not only for the exams performed, but the effects of the Deficit Reduction Act and changes in Medicare reimbursement, both of which contribute to a rather complex financial picture.
Data from the study will be further analyzed to look more formally at costs and interventions. Overall, "revenue from CTA at least compensated for the decreases in nuclear and treadmill testing, while interventional income fell by approximately 15%," Budoff said.
From the physician's perspective, CT is much quicker than alternative studies. "I can be talking to a patient in my clinic and send him for a CTA within 10 minutes," he said. "There's no fasting, you (don't) have to avoid caffeine for 12 hours and all the other stuff. You can get the study done and have the results in 30 minutes."
About 60% of the clinic's CTA studies are now performed using prospectively gated low-dose protocols, with the rest undergoing multiphase retrospectively gated studies. The decision depends on the patent's presentation and the wishes of the referring physician.
"We usually try to decide up front if we need functional imaging and then make that decision," Budoff said. Patients who require wall motion assessment, or an abnormal nuclear or stress echocardiography study, are instead referred for dose-modulated retrospectively gated CT angiography.
"We often do a CTA with wall motion (analysis) in order to get a better assessment of the ejection fraction," he said. "When the ejection fraction is low, CTA tends to assess it better than nuclear and most echo exams."
By Eric Barnes
AuntMinnie.com staff writer
April 1, 2008
Related Reading
Prospective gating drops cardiac CT radiation dose, March 10, 2008
ACCURACY trial compares coronary CTA to angiography, January 18, 2008
CTA predicts mortality, shows variable risk per vessel, December 7, 2007
Sublingual nitroglycerin improves coronary CTA, December 31, 2007
Low-dose coronary CTA diagnoses most patients, November 28, 2007
Copyright © 2008 AuntMinnie.com